

Clinical utility of cardiovascular magnetic resonance in hypertrophic cardiomyopathy
- PMID: 22296938
- PMCID: PMC3293092
- DOI: 10.1186/1532-429X-14-13
Clinical utility of cardiovascular magnetic resonance in hypertrophic cardiomyopathy
Abstract
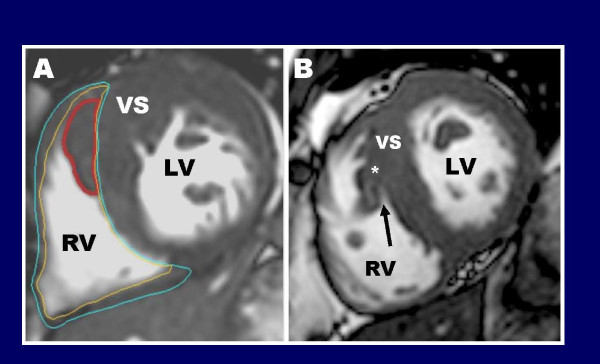
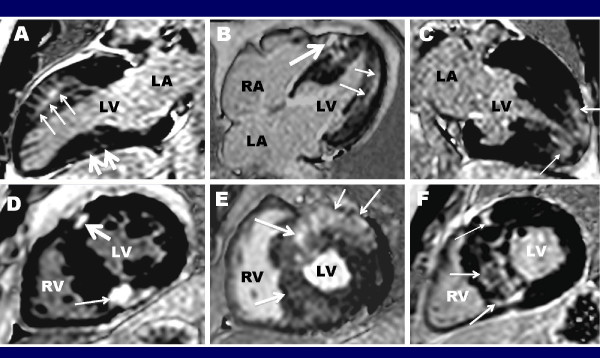
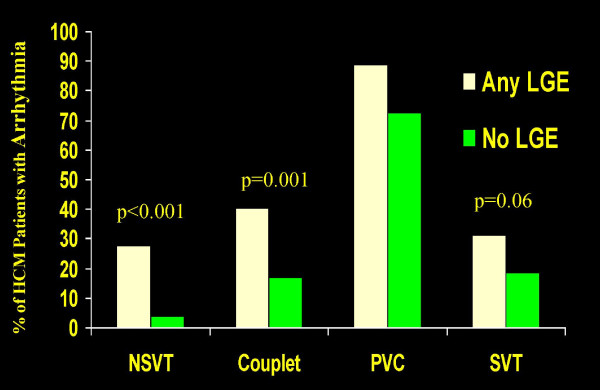
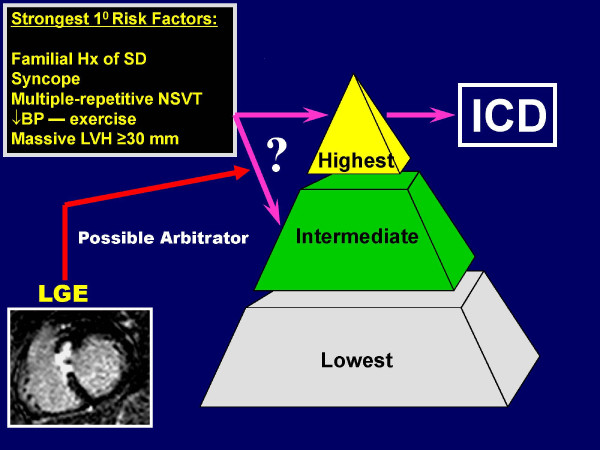
Hypertrophic cardiomyopathy (HCM) is characterized by substantial genetic and phenotypic heterogeneity, leading to considerable diversity in clinical course including the most common cause of sudden death in young people and a determinant of heart failure symptoms in patients of any age. Traditionally, two-dimensional echocardiography has been the most reliable method for establishing a clinical diagnosis of HCM. However, cardiovascular magnetic resonance (CMR), with its high spatial resolution and tomographic imaging capability, has emerged as a technique particularly well suited to characterize the diverse phenotypic expression of this complex disease. For example, CMR is often superior to echocardiography for HCM diagnosis, by identifying areas of segmental hypertrophy (ie., anterolateral wall or apex) not reliably visualized by echocardiography (or underestimated in terms of extent). High-risk HCM patient subgroups identified with CMR include those with thin-walled scarred LV apical aneurysms (which prior to CMR imaging in HCM remained largely undetected), end-stage systolic dysfunction, and massive LV hypertrophy. CMR observations also suggest that the cardiomyopathic process in HCM is more diffuse than previously regarded, extending beyond the LV myocardium to include thickening of the right ventricular wall as well as substantial morphologic diversity with regard to papillary muscles and mitral valve. These findings have implications for management strategies in patients undergoing invasive septal reduction therapy. Among HCM family members, CMR has identified unique phenotypic markers of affected genetic status in the absence of LV hypertrophy including: myocardial crypts, elongated mitral valve leaflets and late gadolinium enhancement. The unique capability of contrast-enhanced CMR with late gadolinium enhancement to identify myocardial fibrosis has raised the expectation that this may represent a novel marker, which may enhance risk stratification. At this time, late gadolinium enhancement appears to be an important determinant of adverse LV remodeling associated with systolic dysfunction. However, the predictive significance of LGE for sudden death is incompletely resolved and ultimately future large prospective studies may provide greater insights into this issue. These observations underscore an important role for CMR in the contemporary assessment of patients with HCM, providing important information impacting diagnosis and clinical management strategies.
Figures
References
-
- Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA. 2002;287:1308–20. - PubMed
-
- Wigle ED, Rakowski H, Kimball BP, Williams WG. Hypertrophic cardiomyopathy. Clinical spectrum and treatment. Circulation. 1995;92:1680–92. - PubMed
-
- Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, Shah PM, Spencer WH, Spirito P, Ten Cate FJ, Wigle ED. American College of Cardiology/European Society of Cardiology clinical expert consensus document on hypertrophic cardiomyopathy. A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines. J Am Coll Cardiol. 2003;42:1687–713. - PubMed
-
- Alcalai R, Seidman JG, Seidman CE. Genetic basis of hypertrophic cardiomyopathy: from bench to the clinics. J Cardiovasc Electrophysiol. 2008;19:104–10. - PubMed
-
- Seidman JG, Seidman C. The genetic basis for cardiomyopathy: from mutation identification to mechanistic paradigms. Cell. 2001;104:557–67. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
