

Pros and cons for C4d as a biomarker
- PMID: 22297669
- PMCID: PMC3771104
- DOI: 10.1038/ki.2011.497
Pros and cons for C4d as a biomarker
Abstract
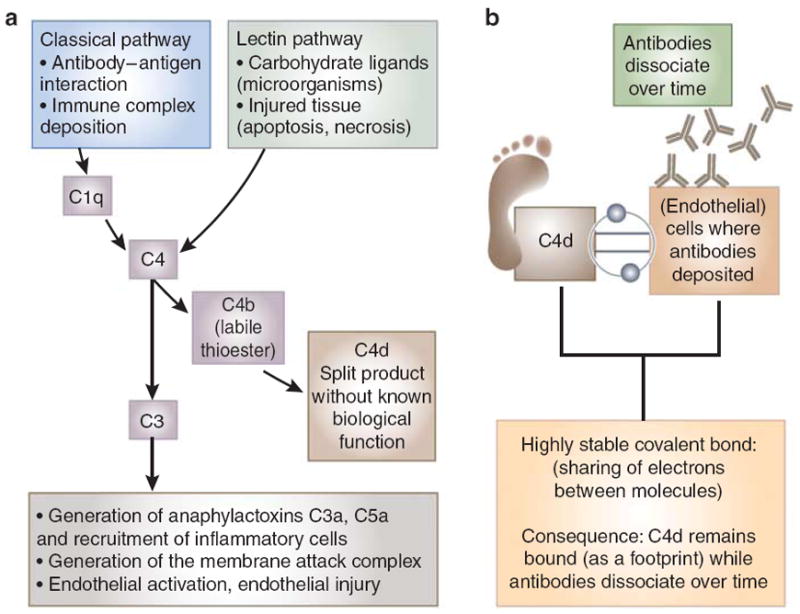
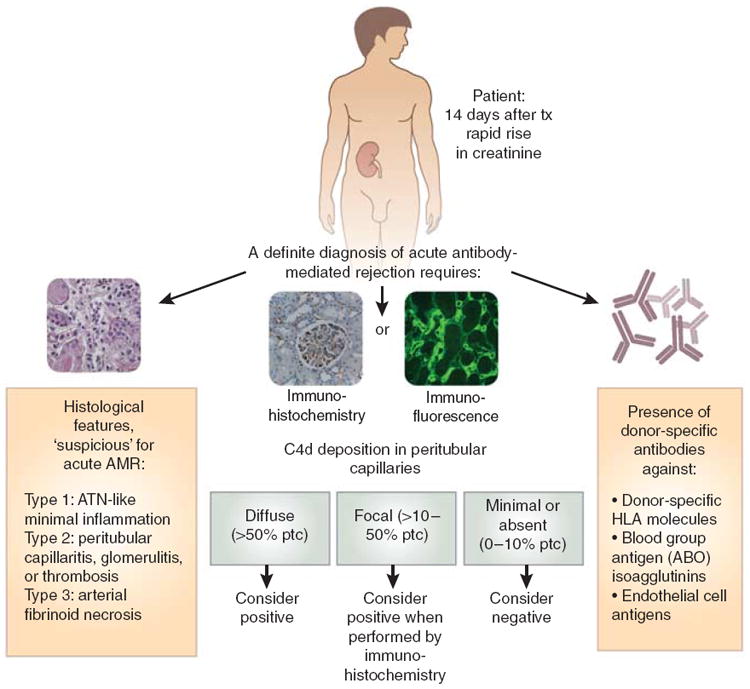
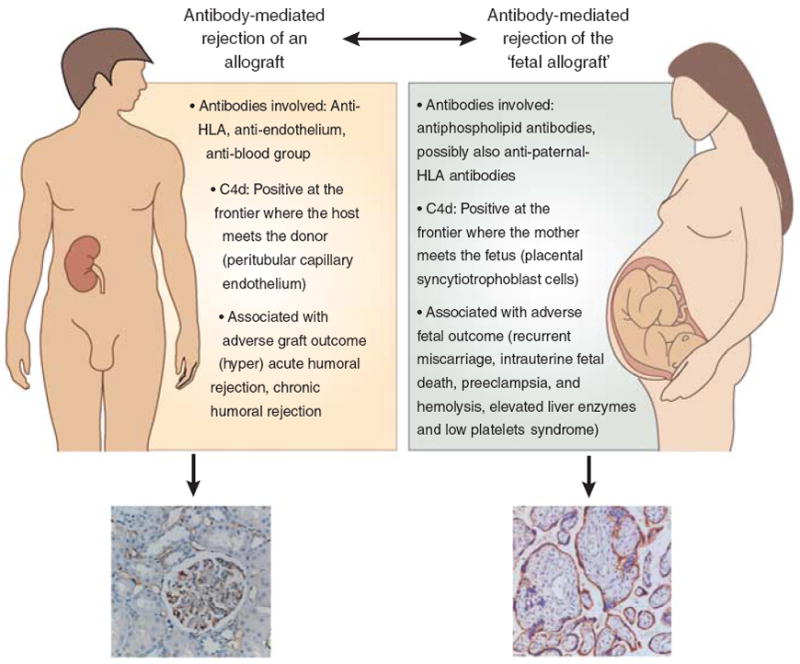
The introduction of C4d in daily clinical practice in the late nineties aroused an ever-increasing interest in the role of antibody-mediated mechanisms in allograft rejection. As a marker of classical complement activation, C4d made it possible to visualize the direct link between anti-donor antibodies and tissue injury at sites of antibody binding in a graft. With the expanding use of C4d worldwide several limitations of C4d were identified. For instance, in ABO-incompatible transplantations C4d is present in the majority of grafts but this seems to point at 'graft accommodation' rather than antibody-mediated rejection. C4d is now increasingly recognized as a potential biomarker in other fields where antibodies can cause tissue damage, such as systemic autoimmune diseases and pregnancy. In all these fields, C4d holds promise to detect patients at risk for the consequences of antibody-mediated disease. Moreover, the emergence of new therapeutics that block complement activation makes C4d a marker with potential to identify patients who may possibly benefit from these drugs. This review provides an overview of the past, present, and future perspectives of C4d as a biomarker, focusing on its use in solid organ transplantation and discussing its possible new roles in autoimmunity and pregnancy.
Conflict of interest statement
All the authors declared no competing interests.
Figures
Comment in
-
C4d deposits on erythrocytes (EC4d): a new biomarker of antibody-mediated rejection in kidney transplantation.Kidney Int. 2012 Aug;82(4):490-1. doi: 10.1038/ki.2012.200. Kidney Int. 2012. PMID: 22846818 No abstract available.
References
-
- Nickeleit V, Mihatsch MJ. Kidney transplants, antibodies and rejection: is C4d a magic marker? Nephrol Dial Transplant. 2003;18:2232–2239. - PubMed
-
- Sis B, Halloran PF. Endothelial transcripts uncover a previously unknown phenotype: C4d-negative antibody-mediated rejection. Curr Opin Organ Transplant. 2010;15:42–48. - PubMed
-
- Regele H, Bohmig GA, Habicht A, et al. Capillary deposition of complement split product C4d in renal allografts is associated with basement membrane injury in peritubular and glomerular capillaries: a contribution of humoral immunity to chronic allograft rejection. J Am Soc Nephrol. 2002;13:2371–2380. - PubMed
-
- Berger SP, Roos A, Daha MR. Complement and the kidney: what the nephrologist needs to know in 2006? Nephrol Dial Transplant. 2005;20:2613–2619. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
