

Mechanisms of alloimmunization and subsequent bone marrow transplantation rejection induced by platelet transfusion in a murine model
- PMID: 22300526
- PMCID: PMC4296674
- DOI: 10.1111/j.1600-6143.2011.03959.x
Mechanisms of alloimmunization and subsequent bone marrow transplantation rejection induced by platelet transfusion in a murine model
Abstract
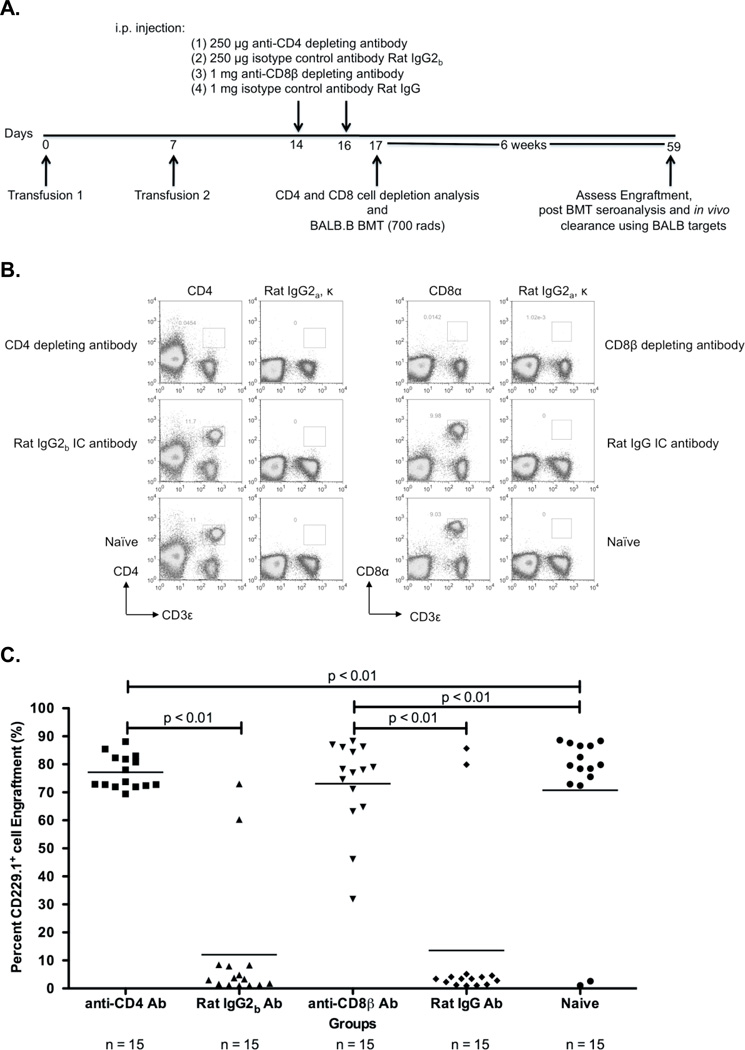
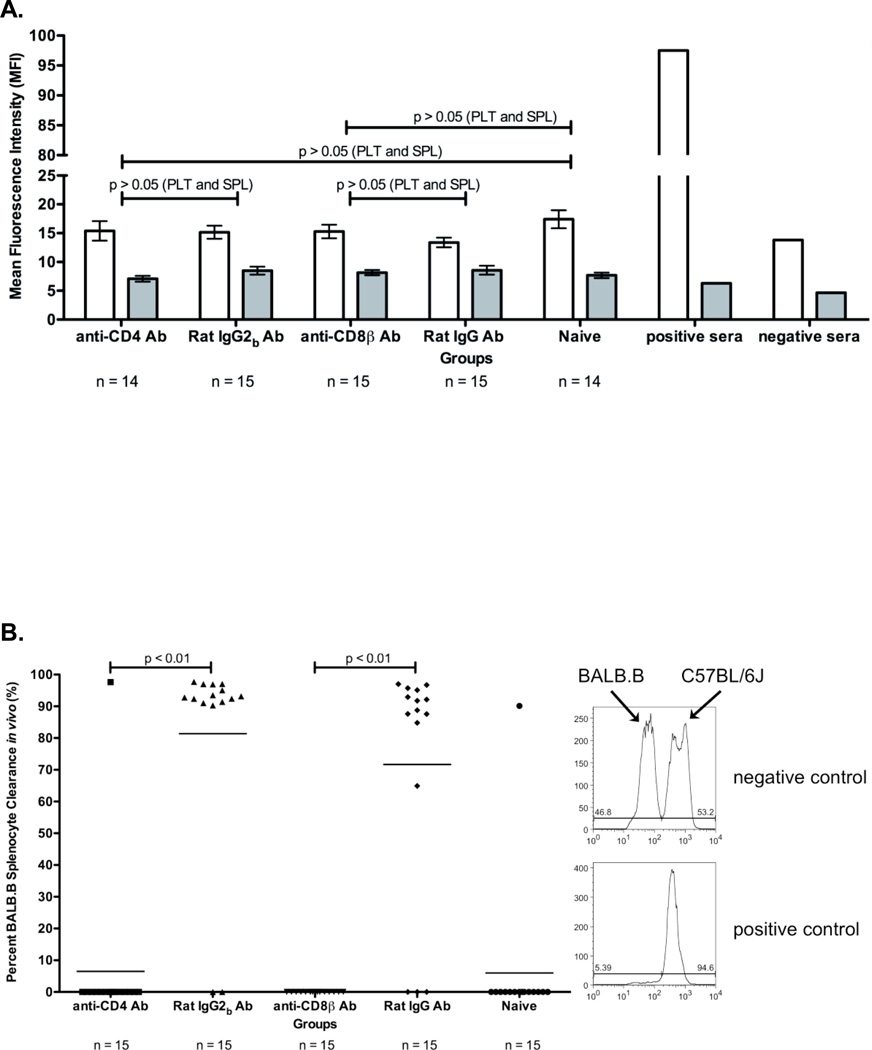
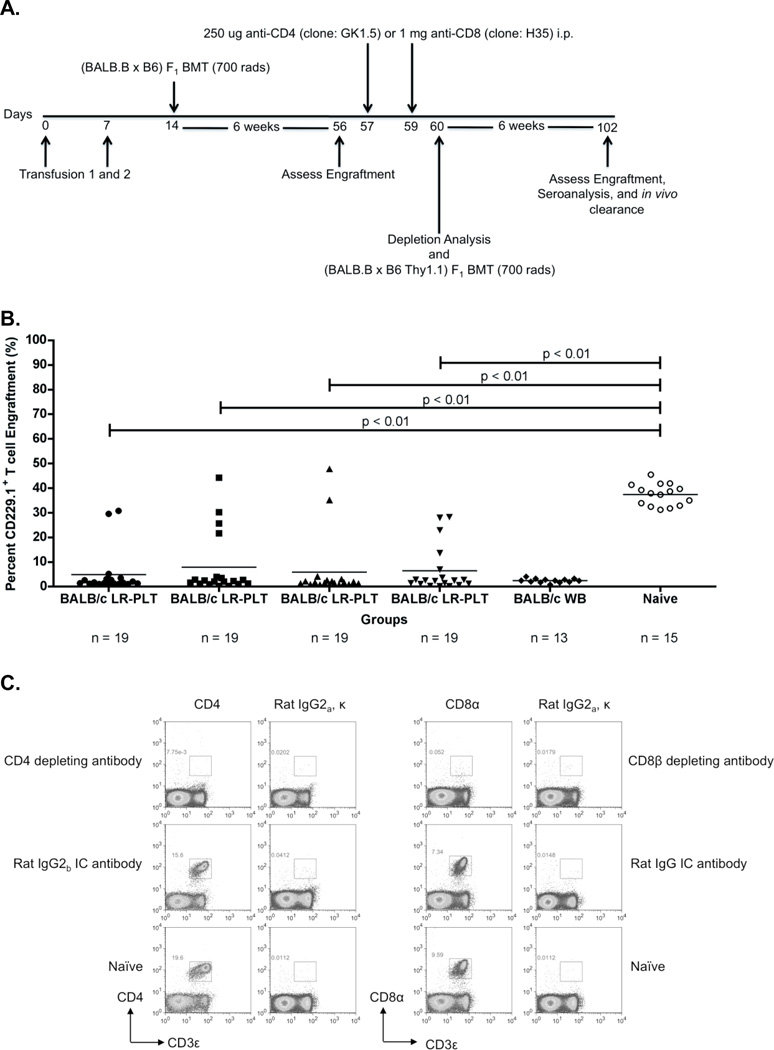
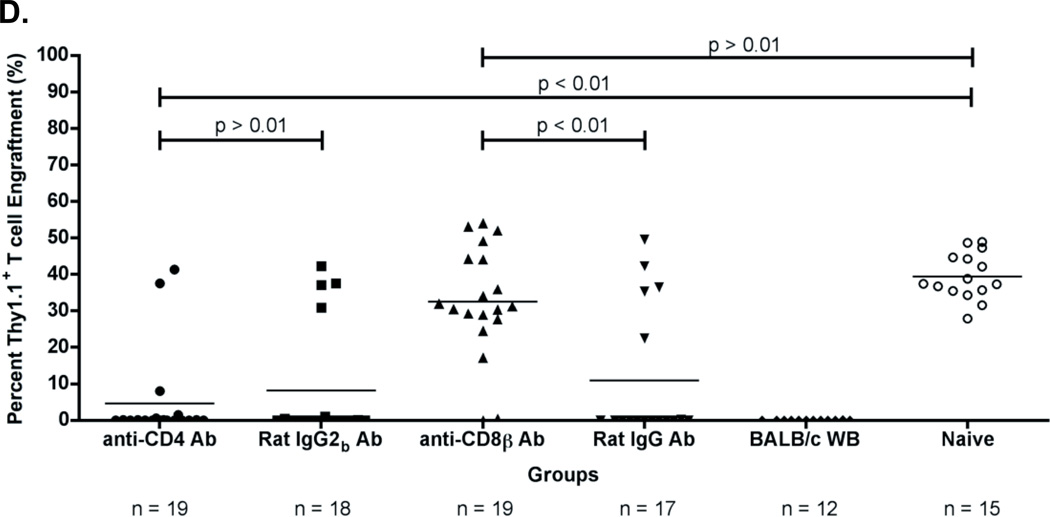
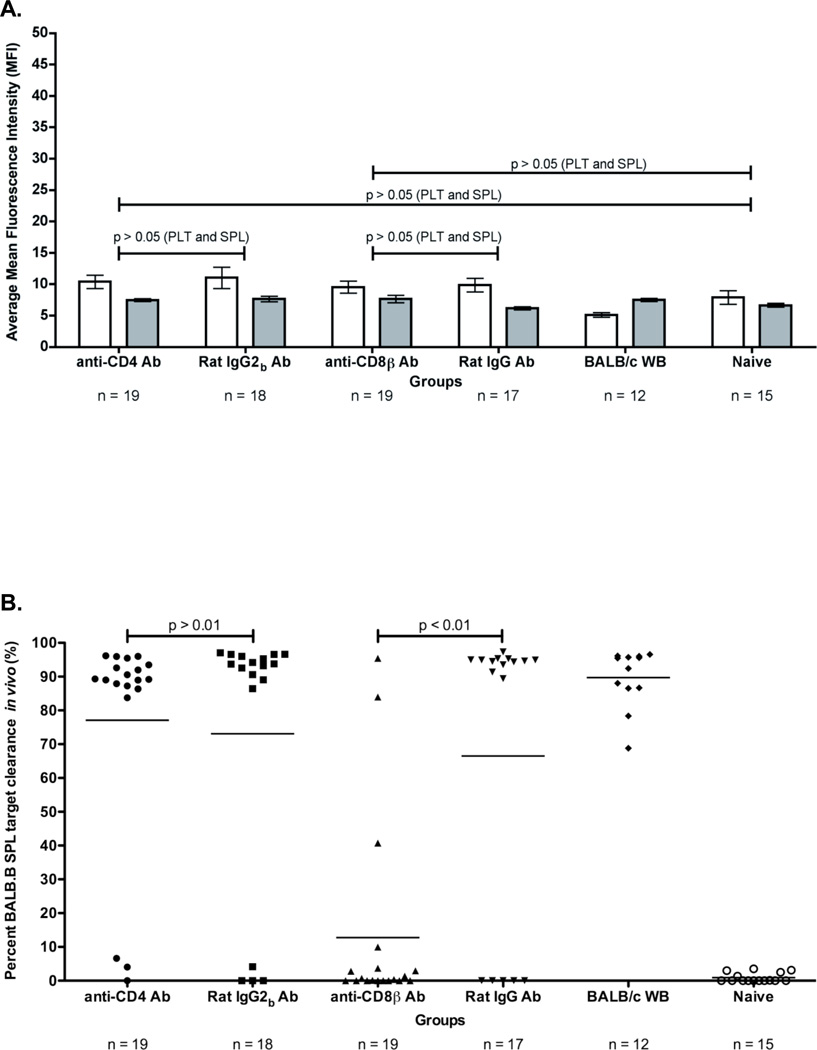
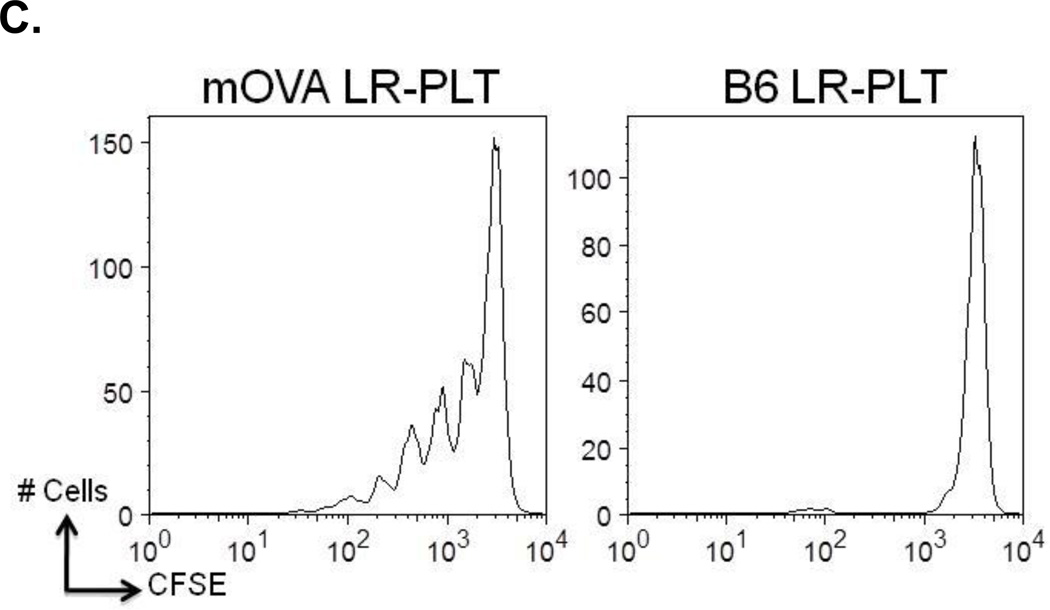
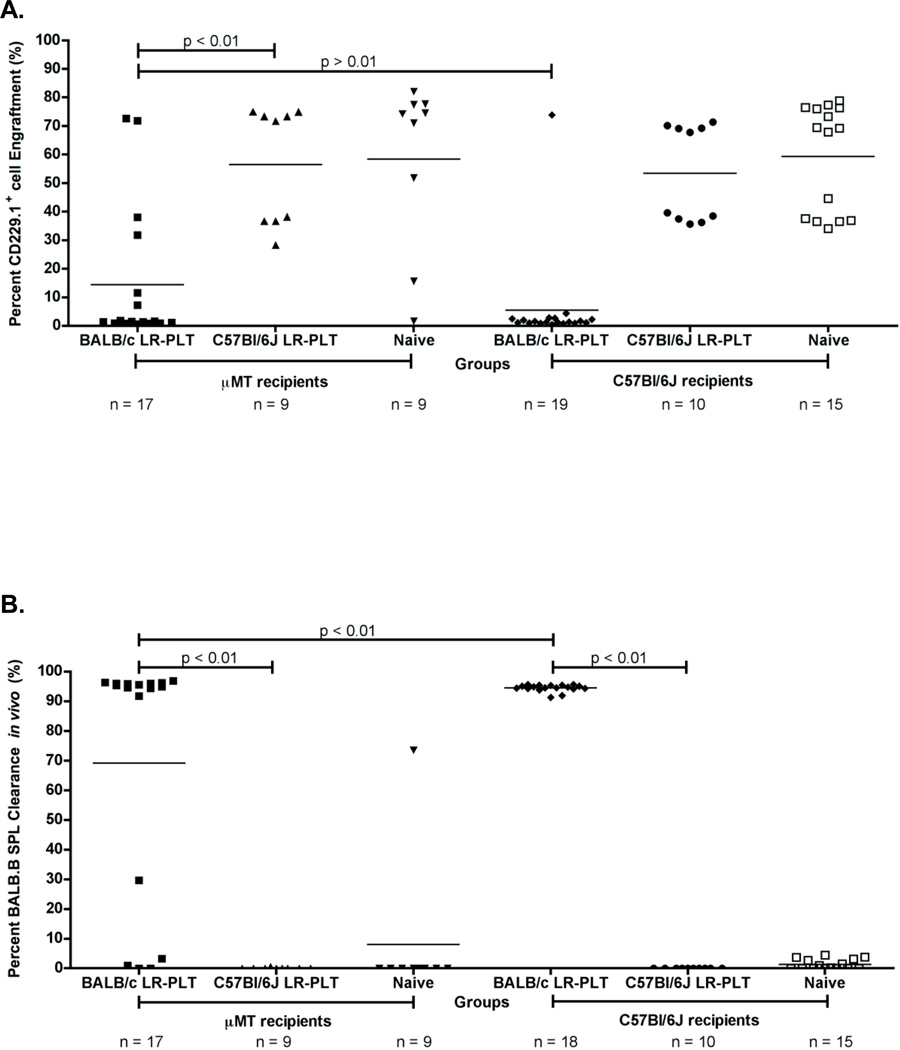
For many nonmalignant hematological disorders, HLA-matched bone marrow transplantation (BMT) is curative. However, due to lack of neoplasia, the toxicity of stringent conditioning regimens is difficult to justify, and reduced intensity conditioning is used. Unfortunately, current reduced intensity regimens have high rates of BMT rejection. We have recently reported in a murine model that mHAs on transfused platelet products induce subsequent BMT rejection. Most nonmalignant hematological disorders require transfusion support prior to BMT and the rate of BMT rejection in humans correlates with the number of transfusions given. Herein, we perform a mechanistic analysis of platelet transfusion-induced BMT rejection and report that unlike exposure to alloantigens during transplantation, platelet transfusion primes alloimmunity but does not stimulate full effector function. Subsequent BMT is itself an additional and distinct immunizing event, which does not induce rejection without antecedent priming from transfusion. Both CD4(+) and CD8(+) T cells are required for priming during platelet transfusion, but only CD8(+) T cells are required for BMT rejection. In neither case are antibodies required for rejection to occur.
© Copyright 2012 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
Figures
Similar articles
-
Transfusion-induced bone marrow transplant rejection due to minor histocompatibility antigens.Transfus Med Rev. 2013 Oct;27(4):241-8. doi: 10.1016/j.tmrv.2013.08.002. Epub 2013 Oct 3. Transfus Med Rev. 2013. PMID: 24090731 Free PMC article. Review.
-
Transfusion of minor histocompatibility antigen-mismatched platelets induces rejection of bone marrow transplants in mice.J Clin Invest. 2009 Sep;119(9):2787-94. doi: 10.1172/JCI39590. Epub 2009 Aug 10. J Clin Invest. 2009. PMID: 19726874 Free PMC article.
-
CTLA4-Ig prevents alloantibody production and BMT rejection in response to platelet transfusions in mice.Transfusion. 2012 Oct;52(10):2209-19. doi: 10.1111/j.1537-2995.2011.03550.x. Epub 2012 Feb 10. Transfusion. 2012. PMID: 22321003 Free PMC article.
-
Minor histocompatibility antigens on transfused leukoreduced units of red blood cells induce bone marrow transplant rejection in a mouse model.Blood. 2009 Sep 10;114(11):2315-22. doi: 10.1182/blood-2009-04-214387. Epub 2009 Jun 12. Blood. 2009. PMID: 19525479 Free PMC article.
-
Alloreactivity and the predictive value of anti-recipient specific interleukin 2 producing helper T lymphocyte precursor frequencies for alloreactivity after bone marrow transplantation.Dan Med Bull. 2002 May;49(2):89-108. Dan Med Bull. 2002. PMID: 12064093 Review.
Cited by
-
Pathophysiology of Alloimmunization.Transfus Med Hemother. 2020 Apr;47(2):152-159. doi: 10.1159/000501861. Epub 2019 Aug 6. Transfus Med Hemother. 2020. PMID: 32355475 Free PMC article.
-
Nephro and neurotoxicity of calcineurin inhibitors and mechanisms of rejections: A review on tacrolimus and cyclosporin in organ transplantation.J Nephropathol. 2012 Apr;1(1):23-30. doi: 10.5812/jnp.6. Epub 2012 Apr 5. J Nephropathol. 2012. PMID: 24475383 Free PMC article. Review.
-
Marginal Zone B Cells Induce Alloantibody Formation Following RBC Transfusion.Front Immunol. 2018 Nov 16;9:2516. doi: 10.3389/fimmu.2018.02516. eCollection 2018. Front Immunol. 2018. PMID: 30505302 Free PMC article.
-
Transfusion-induced bone marrow transplant rejection due to minor histocompatibility antigens.Transfus Med Rev. 2013 Oct;27(4):241-8. doi: 10.1016/j.tmrv.2013.08.002. Epub 2013 Oct 3. Transfus Med Rev. 2013. PMID: 24090731 Free PMC article. Review.
-
Red blood cell transfusions are associated with HLA class I but not H-Y alloantibodies in children with sickle cell disease.Br J Haematol. 2015 Jul;170(2):247-56. doi: 10.1111/bjh.13424. Epub 2015 Apr 19. Br J Haematol. 2015. PMID: 25891976 Free PMC article.
References
-
- Bhatia M, Walters MC. Hematopoietic cell transplantation for thalassemia and sickle cell disease: past, present and future. Bone Marrow Transplant. 2008;41(2):109–117. - PubMed
-
- Horan JT, Liesveld JL, Fenton P, Blumberg N, Walters MC. Hematopoietic stem cell transplantation for multiply transfused patients with sickle cell disease and thalassemia after low-dose total body irradiation, fludarabine, and rabbit anti-thymocyte globulin. Bone Marrow Transplant. 2005;35(2):171–177. - PubMed
-
- Marsh JC, Ball SE, Darbyshire P, Gordon-Smith EC, Keidan AJ, Martin A, et al. Guidelines for the diagnosis and management of acquired aplastic anaemia. Br J Haematol. 2003;123(5):782–801. - PubMed
-
- Or R, Aker M, Shapira MY, Resnick I, Bitan M, Samuel S, et al. Allogeneic stem cell transplantation for the treatment of diseases associated with a deficiency in bone marrow products. Springer Semin Immunopathol. 2004;26(1–2):133–142. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
