

Incidence of and risk factors for sudden cardiac death in children with dilated cardiomyopathy: a report from the Pediatric Cardiomyopathy Registry
- PMID: 22300696
- PMCID: PMC3280885
- DOI: 10.1016/j.jacc.2011.10.878
Incidence of and risk factors for sudden cardiac death in children with dilated cardiomyopathy: a report from the Pediatric Cardiomyopathy Registry
Abstract
Objectives: The purpose of this study was to establish the incidence of and risk factors for sudden cardiac death (SCD) in pediatric dilated cardiomyopathy (DCM).
Background: The incidence of SCD in children with DCM is unknown. The ability to predict patients at high risk of SCD will help to define who may benefit most from implantable cardioverter-defibrillators.
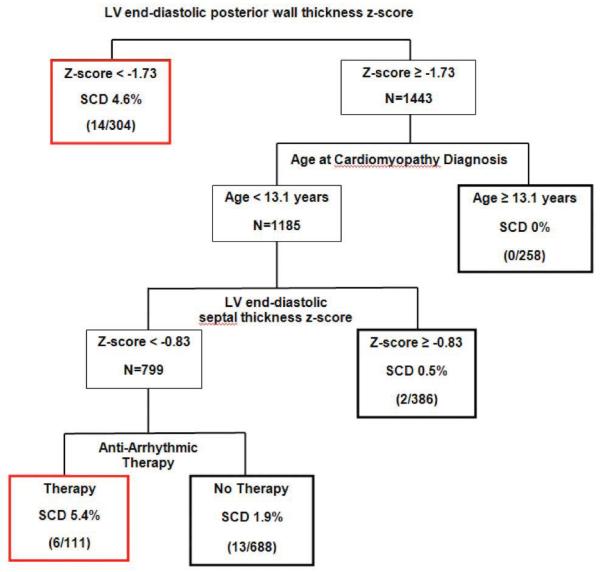
Methods: The cohort was 1,803 children in the PCMR (Pediatric Cardiomyopathy Registry) with a diagnosis of DCM from 1990 to 2009. Cumulative incidence competing-risks event rates were estimated. We achieved risk stratification using Classification and Regression Tree methodology.
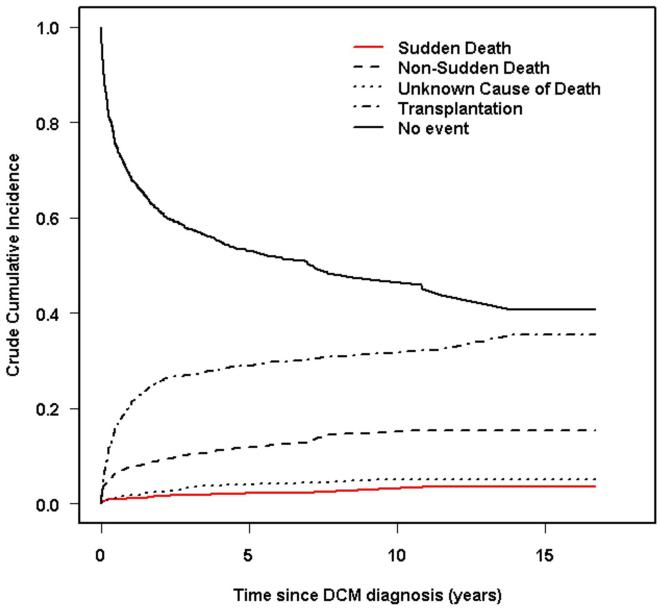
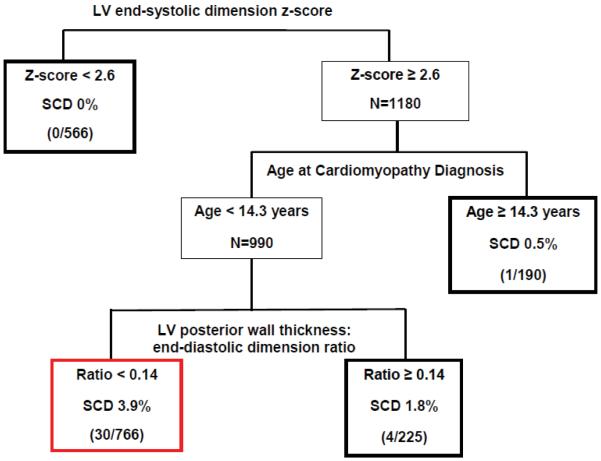
Results: The 5-year incidence rates were 29% for heart transplantation, 12.1% non-SCD, 4.0% death from unknown cause, and 2.4% for SCD. Of 280 deaths, 35 were SCD, and the cause was unknown for 56. The 5-year incidence rate for SCD incorporating a subset of the unknown deaths is 3%. Patients receiving antiarrhythmic medication were at higher risk of SCD (hazard ratio: 3.0, 95% confidence interval: 1.1 to 8.3, p = 0.025). A risk stratification model based on most recent echocardiographic values had 86% sensitivity and 57% specificity. Thirty of 35 SCDs occurred in patients who met all these criteria: left ventricular (LV) end-systolic dimension z-score >2.6, age at diagnosis younger than 14.3 years, and the LV posterior wall thickness to end-diastolic dimension ratio <0.14. Sex, ethnicity, cause of DCM, and family history were not associated with SCD.
Conclusions: The 5-year incidence rate of SCD in children with DCM is 3%. A risk stratification rule (86% sensitivity) included age at diagnosis younger than 14.3 years, LV dilation, and LV posterior wall thinning. Patients who consistently meet these criteria should be considered for implantable cardioverter-defibrillator placement.
Trial registration: ClinicalTrials.gov NCT00005391.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Johnson RA, Palacious I. Dilated cardiomyopathy of the adult. N Engl J Med. 1996;334:493–9.
-
- Kadish A, Dyer A, Daubert JP, et al. Defibrillators in Non-Ischemic Cardiomyopathy Treatment Evaluation (DEFINITE) Investigators Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med. 2004;350:2151–8. - PubMed
-
- Bänsch D, Antz M, Boczor S, et al. Primary prevention of sudden cardiac death in idiopathic dilated cardiomyopathy: the Cardiomyopathy Trial (CAT) Circulation. 2002;105:1453–8. - PubMed
-
- Bardy G, Lee KL, Mark DB, et al. Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. - PubMed
-
- Epstein AE, DiMarco JP, Ellenbogen KA, et al. American Association for Thoracic Surgery, Society of Thoracic Surgeons. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons J Am Coll Cardiol. 2008;51:e1–e62. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
