

Zuckerkandl tubercle of the thyroid: a common imaging finding that may mimic pathology
- PMID: 22300934
- PMCID: PMC8013239
- DOI: 10.3174/ajnr.A2914
Zuckerkandl tubercle of the thyroid: a common imaging finding that may mimic pathology
Abstract
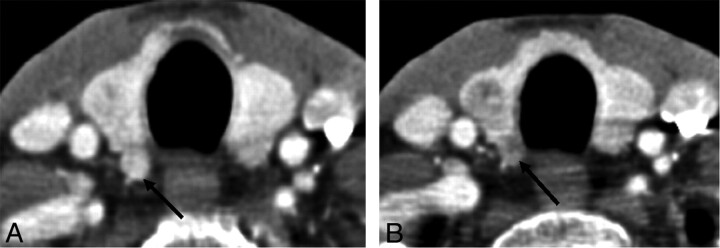
Background and purpose: The posterior thyroid tubercle, also known as ZT, is an important surgical landmark due to its close proximity to the recurrent laryngeal nerve. A recent case of ZT with a nodular configuration caused clinical concern but was shown on biopsy to be normal thyroid tissue. The purpose of this study was to review a series of CT neck studies to identify how often ZT-specifically, a nodular subtype-was present.
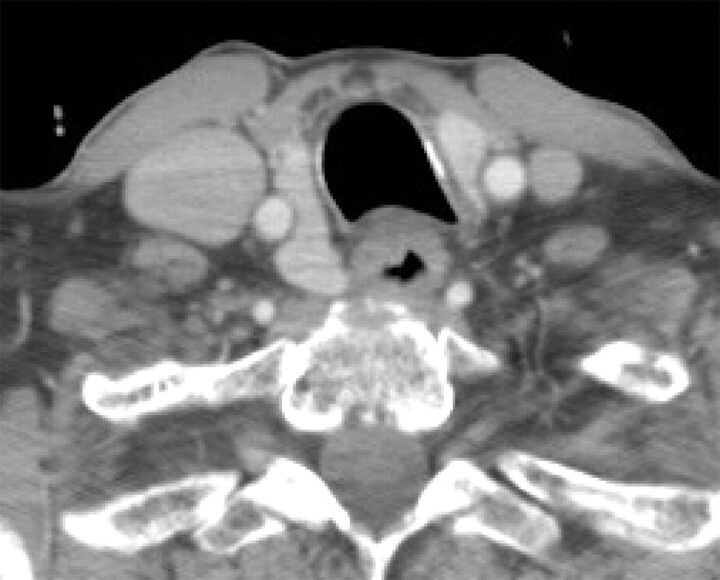
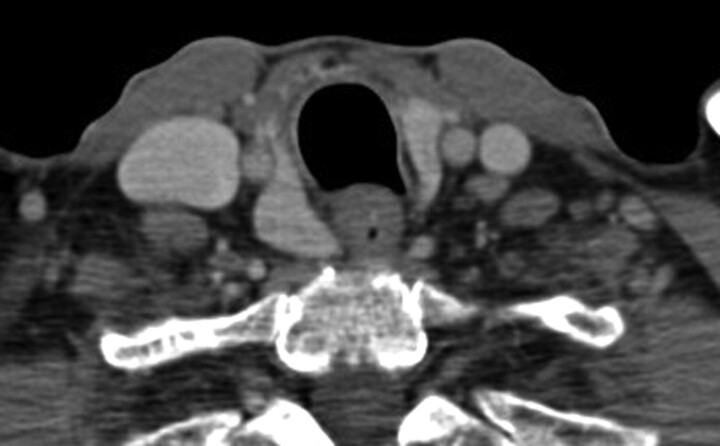
Materials and methods: A total of 96 neck CTs from sequential patients were retrospectively identified from January 2010 to July 2010. ZT was defined on imaging as a thyroid lobe extending posterior to the tracheoesophageal groove. A nodular subtype was defined as having a narrowed neck at the level of the tracheoesophageal groove.
Results: There were 31 women and 45 men (mean age of 56.1 years, range 22-100 years) who met inclusion criteria. Sixty-seven patients had thyroid glands that extended posterior to the tracheoesophageal groove at CT imaging; this finding was bilateral in 43 patients, more commonly on the right (60 versus 49). Thirty-two of these patients (42.1%; 16 male, 16 female) had a nodular subtype.
Conclusions: ZT is an important surgical landmark of the thyroid that has important radiologic variations. It has a nodular shape in over a third of CT neck studies in our series. Recognition of this feature of the thyroid gland at CT imaging can obviate the need for biopsy and avoid potential recurrent laryngeal nerve injury.
Figures







References
-
- Mirilas P, Skandalakis JE. Zuckerkandl's tubercle: Hannibal ad Portas. Am Coll Surg 2003;196;5:796–801 - PubMed
-
- Yalcin B, Tatar I, Ozan H. The Zuckerkandl tubercle and the recurrent laryngeal nerve. Am J Surg 2008;196:311–12 - PubMed
-
- Costanzo M, Caruso LA, Veroux M, et al. . The lobe of Zuckerkandl: an important sign of recurrent laryngeal nerve. Ann Ital Chir 2005;76:337–40, discussion 340–41 - PubMed
-
- Musajo FG, Mangiante G, Ischia A, et al. . Zuckerkandl tubercle of the thyroid gland (anatomo-surgical study: preliminary considerations). Chir Ital 1989;41:129–36 - PubMed
-
- Buck RT, Siddiqui AR. Thyroid abnormality secondary to tortuous carotid artery. Eur J Nucl Med 1986;12:51–52 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous