

Results for primary bypass versus primary angioplasty/stent for intermittent claudication due to superficial femoral artery occlusive disease
- PMID: 22301210
- PMCID: PMC3319263
- DOI: 10.1016/j.jvs.2011.10.128
Results for primary bypass versus primary angioplasty/stent for intermittent claudication due to superficial femoral artery occlusive disease
Abstract
Background: Percutaneous transluminal angioplasty ± stent (PTA/S) and surgical bypass are both accepted treatments for claudication due to superficial femoral artery (SFA) occlusive disease. However, long-term results comparing these modalities for primary intervention in patients who have had no prior intervention have not been reported. We report our results with 3-year follow-up.
Methods: We reviewed all lower extremity bypass procedures at Beth Israel Deaconess Medical Center from 2001 through 2009 and all PTA/S performed from 2005 through 2009 for claudication. We excluded all limb salvage procedures and included only those that were undergoing their first intervention for claudication due to SFA disease. We recorded patient demographics, comorbidities, perioperative medications, TASC classification, and runoff. Outcomes included complications, restenosis, symptom recurrence, reinterventions, major amputation, and mortality.
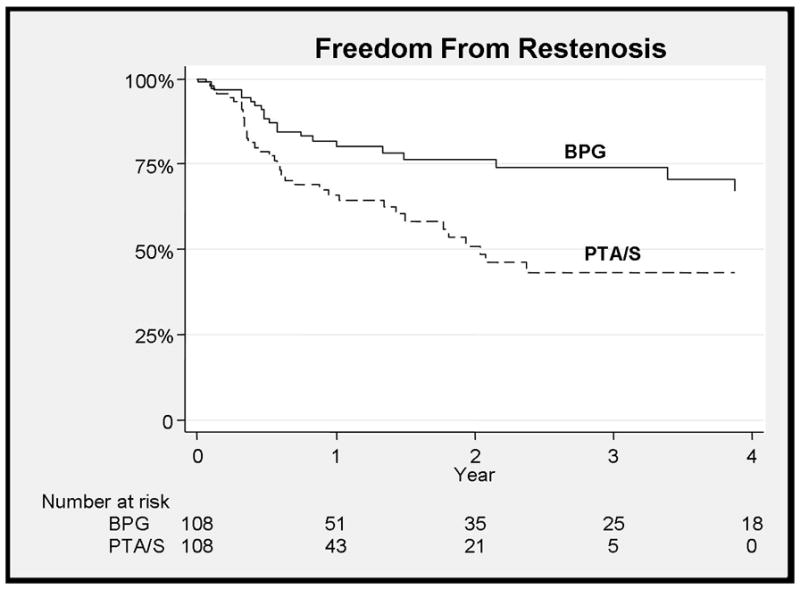
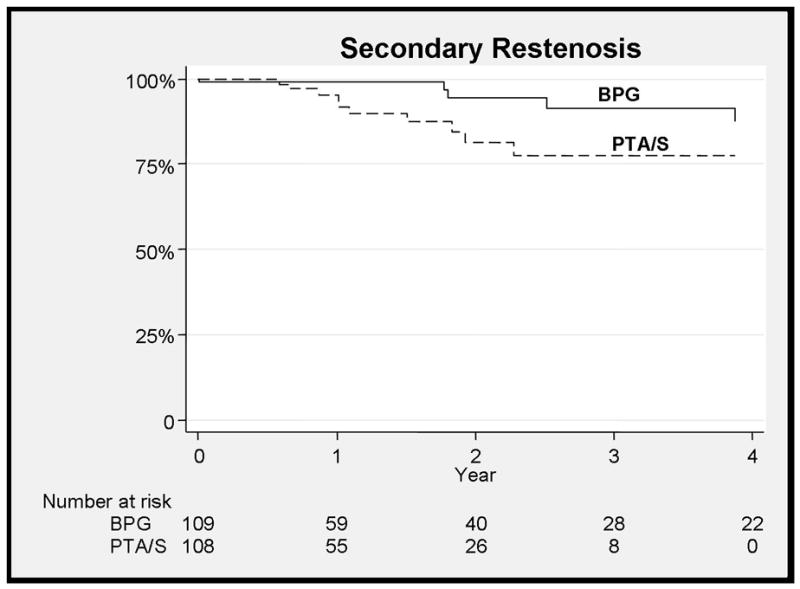
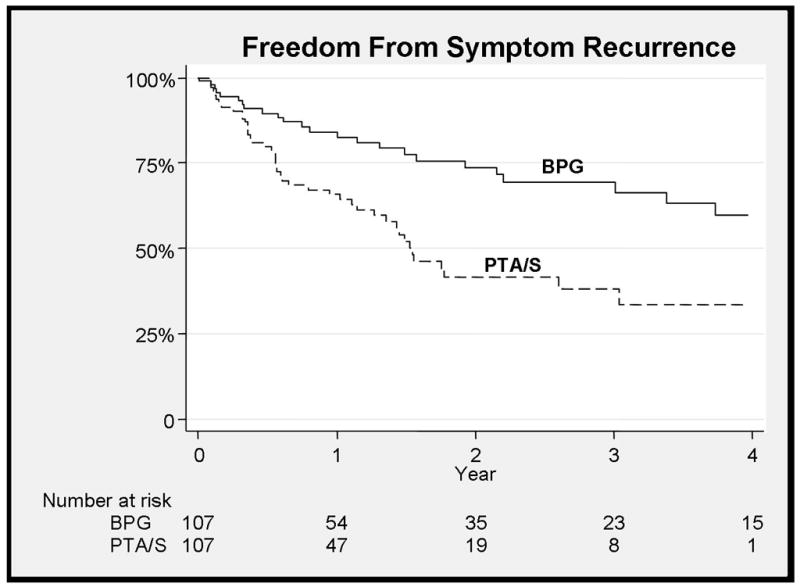
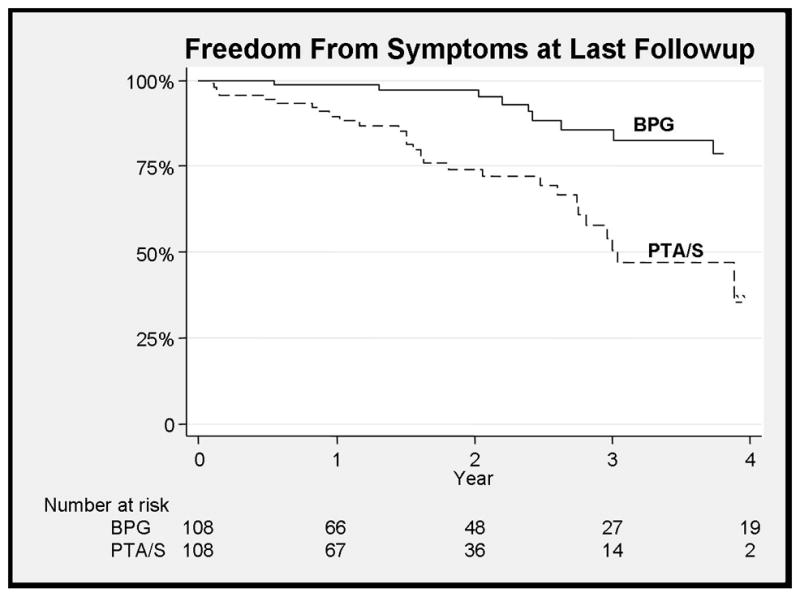
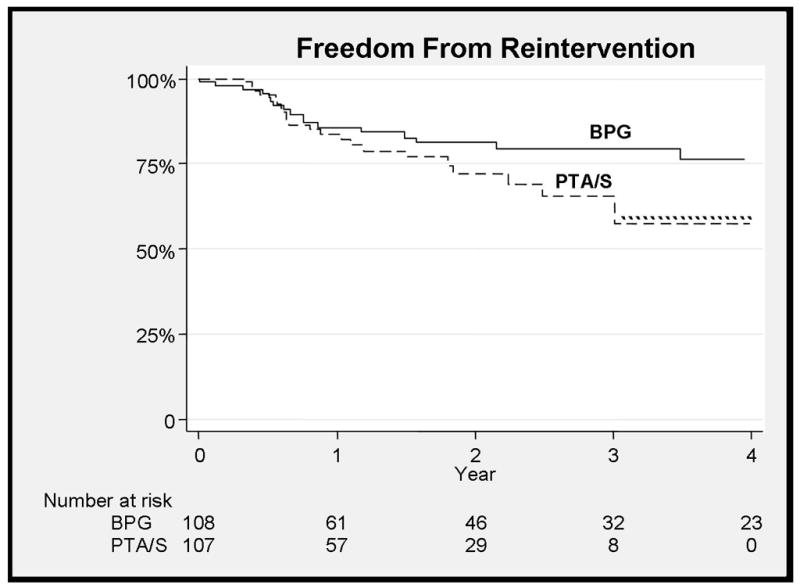
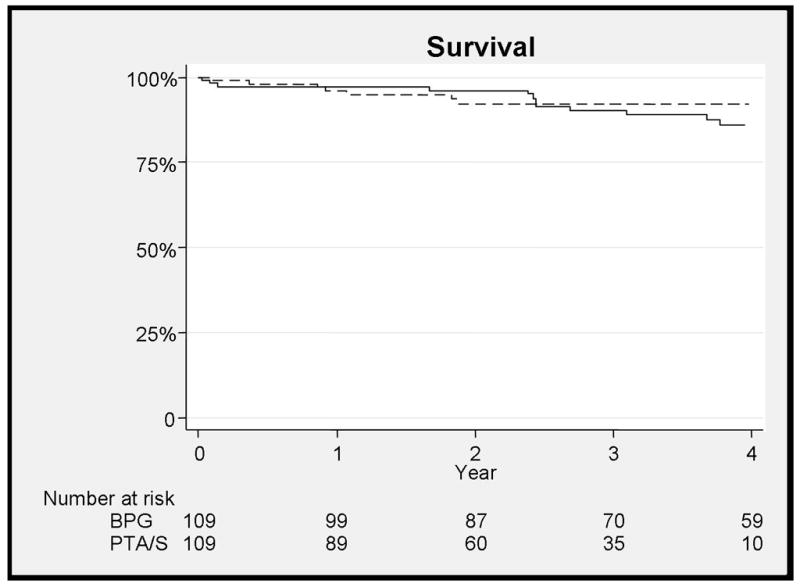
Results: We identified 113 bypass grafts and 105 PTA/S of femoral-popliteal lesions without prior interventions. Bypasses were above the knee in 62% (45% vein) and below the knee in 38% (100% vein). Mean age was 63 (bypass) versus 69 (PTA/S; P < .01). Mean length of stay (LOS) was 3.9 versus 1.2 days (P < .01). Bypass grafts were used less for TASC A (17% vs 40%; P < .01) and more for TASC C (36% vs 11%; P < .01) and TASC D (13% vs 3%; P < .01) lesions. There were no differences in perioperative (2% vs 0%; not significant [NS]) or 3-year mortality (9% vs 8%; NS). Wound infection was higher with bypass (16% vs 0%; P < .01). None involved grafts. Bypass showed improved freedom from restenosis (73% vs 42% at 3 years; hazard ratio [HR], 0.4; 95% confidence interval [CI], .23-.71), symptom recurrence (70% and 36% at 3 years; HR, 0.37; 95% CI, .2-.56), and freedom from symptoms at last follow-up (83% vs 49%; HR, 0.18; 95% CI, .08-.40). There was no difference in freedom from reintervention (77% vs 66% at 3 years; NS). Multivariable analysis of all patients showed that restenosis was predicted by PTA/S (HR, 2.5; 95% CI, 1.4-4.4) and TASC D (HR, 3.7; 95% CI, 3.5-9) lesions. Recurrence of symptoms was similarly predicted by PTA/S (HR, 3.0; 95% CI, 1.8-5) and TASC D lesions (HR, 3.1; 95% CI, 1.4-7). Statin use postoperatively was predictive of patency (HR, 0.6; 95% CI, .35-.97) and freedom from recurrent symptoms (HR, 0.6; 95% CI, .36-.93).
Conclusions: Surgical bypass for the primary treatment of claudication showed improved freedom from restenosis and symptom relief despite treatment of more extensive disease, but was associated with increased LOS and wound infection. Statins improved freedom from restenosis and symptom recurrence overall.
Copyright © 2012 Society for Vascular Surgery. Published by Mosby, Inc. All rights reserved.
Figures
Similar articles
-
Contemporary outcomes after superficial femoral artery angioplasty and stenting: the influence of TASC classification and runoff score.J Vasc Surg. 2008 May;47(5):967-74. doi: 10.1016/j.jvs.2007.12.050. Epub 2008 Apr 18. J Vasc Surg. 2008. PMID: 18372147
-
Results for primary bypass versus primary angioplasty/stent for lower extremity chronic limb-threatening ischemia.J Vasc Surg. 2017 Aug;66(2):466-475. doi: 10.1016/j.jvs.2017.01.024. Epub 2017 Mar 6. J Vasc Surg. 2017. PMID: 28274753 Free PMC article.
-
The treatment of disabling intermittent claudication in patients with superficial femoral artery occlusive disease--decision analysis.J Vasc Surg. 2007 Jun;45(6):1179-84. doi: 10.1016/j.jvs.2007.02.044. J Vasc Surg. 2007. PMID: 17543682
-
Endovascular treatment of lesions in the below-knee popliteal artery.J Vasc Surg. 2014 Aug;60(2):356-61. doi: 10.1016/j.jvs.2014.02.012. Epub 2014 Mar 18. J Vasc Surg. 2014. PMID: 24650745
-
Outcomes of interventions for recurrent disease after endoluminal intervention for superficial femoral artery disease.J Vasc Surg. 2010 Aug;52(2):331-9.e1-2. doi: 10.1016/j.jvs.2010.02.278. Epub 2010 May 15. J Vasc Surg. 2010. PMID: 20478687
Cited by
-
Comparison of morphometric, structural, mechanical, and physiologic characteristics of human superficial femoral and popliteal arteries.Acta Biomater. 2021 Feb;121:431-443. doi: 10.1016/j.actbio.2020.11.025. Epub 2020 Nov 21. Acta Biomater. 2021. PMID: 33227490 Free PMC article.
-
Factors associated with severe lower extremity artery disease in type 2 diabetes based on a large scale claims database in Japan.Sci Rep. 2025 Jun 3;15(1):19358. doi: 10.1038/s41598-025-03797-9. Sci Rep. 2025. PMID: 40461596 Free PMC article.
-
Patient specific characterization of artery and plaque material properties in peripheral artery disease.J Mech Behav Biomed Mater. 2020 Jan;101:103453. doi: 10.1016/j.jmbbm.2019.103453. Epub 2019 Sep 27. J Mech Behav Biomed Mater. 2020. PMID: 31585351 Free PMC article.
-
Major adverse limb events and major adverse cardiac events after contemporary lower extremity bypass and infrainguinal endovascular intervention in patients with claudication.J Vasc Surg. 2018 Dec;68(6):1817-1823. doi: 10.1016/j.jvs.2018.06.193. J Vasc Surg. 2018. PMID: 30470369 Free PMC article.
-
Relationship between regional spending on vascular care and amputation rate.JAMA Surg. 2014 Jan;149(1):34-42. doi: 10.1001/jamasurg.2013.4277. JAMA Surg. 2014. PMID: 24258010 Free PMC article.
References
-
- Schermerhorn ML, Cronenwett JL, Baldwin JC. Open surgical repair versus endovascular therapy for chronic lower-extremity occlusive disease. Annu Rev Med. 2003;54:269–83. Epub 2001 Dec 3. Review. - PubMed
-
- Stewart KJ, Hiatt WR, Regensteiner JG, Hirsch AT. Exercise training for claudication. N Engl J Med. 2002 Dec 12;347(24):1941–51. Review. - PubMed
-
- Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). TASC II Working Group. J Vasc Surg. 2007 Jan;45(Suppl S):S5–67. - PubMed
-
- Nicolaï SP, Hendriks EJ, Prins MH, Teijink JA EXITPAD study group. Optimizing supervised exercise therapy for patients with intermittent claudication. J Vasc Surg. 2010 Nov;52(5):1226–33. Epub 2010 Aug 8. - PubMed
-
- Byrne J, Darling RC, 3rd, Chang BB, Paty PS, Kreienberg PB, Lloyd WE, Leather RP, Shah DM. Infrainguinal arterial reconstruction for claudication: is it worth the risk? An analysis of 409 procedures. J Vasc Surg. 1999 Feb;29(2):259–67. discussion 267–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
