

Gamma heavy-chain disease: defining the spectrum of associated lymphoproliferative disorders through analysis of 13 cases
- PMID: 22301495
- PMCID: PMC3715127
- DOI: 10.1097/PAS.0b013e318240590a
Gamma heavy-chain disease: defining the spectrum of associated lymphoproliferative disorders through analysis of 13 cases
Abstract
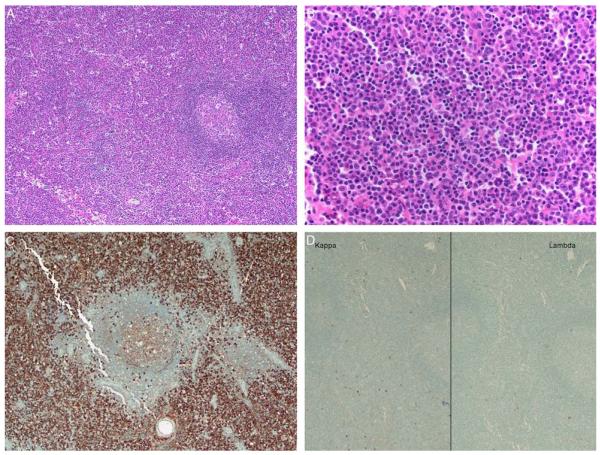
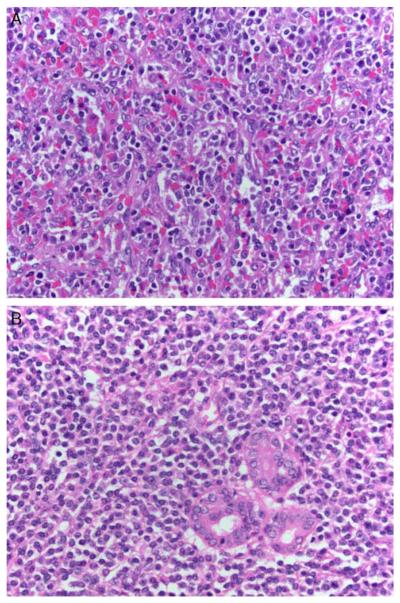
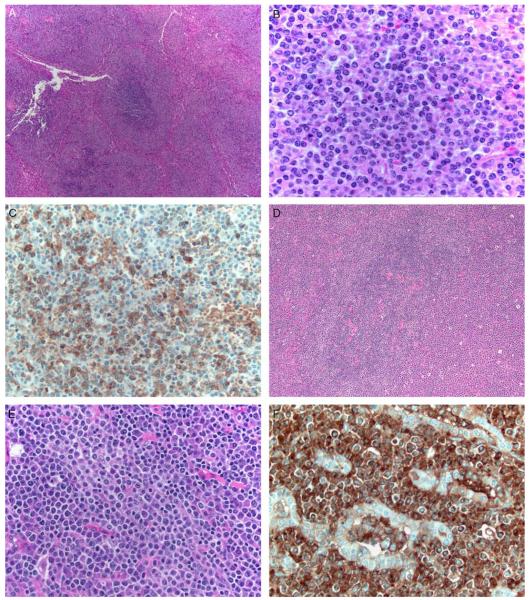
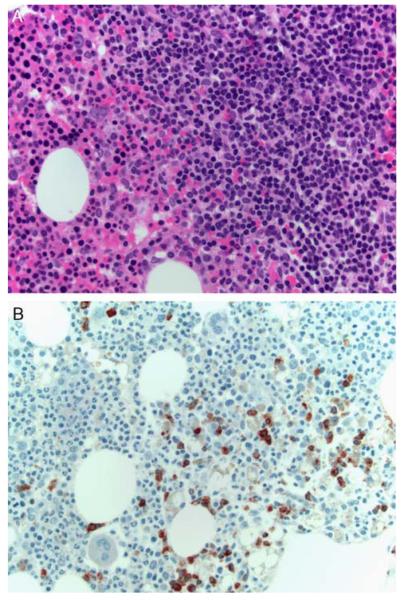
Gamma heavy-chain disease (gHCD) is defined as a lymphoplasmacytic neoplasm that produces an abnormally truncated immunoglobulin gamma heavy-chain protein that lacks associated light chains. There is scant information in the literature regarding the morphologic findings in this rare disorder, but cases have often been reported to resemble lymphoplasmacytic lymphoma (LPL). To clarify the spectrum of lymphoproliferative disorders that may be associated with gHCD, this study reports the clinical, morphologic, and phenotypic findings in 13 cases of gHCD involving lymph nodes (n=7), spleen (n=2), bone marrow (n=8), or other extranodal tissue biopsies (n=3). Clinically, patients showed a female predominance (85%) with frequent occurrence of autoimmune disease (69%). Histologically, 8 cases (61%) contained a morphologically similar neoplasm of small lymphocytes, plasmacytoid lymphocytes, and plasma cells that was difficult to classify with certainty, whereas the remaining 5 cases (39%) showed the typical features of one of several other well-defined entities in the 2008 WHO classification. This report demonstrates that gHCD is associated with a variety of underlying lymphoproliferative disorders but most often shows features that overlap with cases previously reported as "vaguely nodular, polymorphous" LPL. These findings also provide practical guidance for the routine evaluation of small B-cell neoplasms with plasmacytic differentiation that could represent a heavy-chain disease and give suggestions for an improved approach to the WHO classification of gHCD.
Figures
References
-
- Al-Saleem T, Al-Mondhiry H. Immunoproliferative small intestinal disease (IPSID): a model for mature B-cell neoplasms. Blood. 2005;105:2274–2280. - PubMed
-
- Amakawa R, Ohno H, Fukuhara S. t(9;14)(p13;q32) involving the PAX-5 gene: a unique subtype of 14q32 translocation in B cell non-Hodgkin’s lymphoma. Int J Hematol. 1999;69:65–69. - PubMed
-
- Andriko JA, Swerdlow SH, Aguilera NI, et al. Is lymphoplasmacytic lymphoma/immunocytoma a distinct entity? A clinicopathologic study of 20 cases. Am J Surg Pathol. 2001;25:742–751. - PubMed
-
- Cogne M, Bakhshi A, Korsmeyer SJ, et al. Gene mutations and alternate RNA splicing result in truncated Ig L chains in human gamma H chain disease. J Immunol. 1988;141:1738–1744. - PubMed
-
- Cook JR, Aguilera NI, Reshmi-Skarja S, et al. Lack of PAX5 rearrangements in lymphoplasmacytic lymphomas: reassessing the reported association with t(9;14) Hum Pathol. 2004;35:447–454. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
