

Rare adipose disorders (RADs) masquerading as obesity
- PMID: 22301856
- PMCID: PMC4010336
- DOI: 10.1038/aps.2011.153
Rare adipose disorders (RADs) masquerading as obesity
Abstract
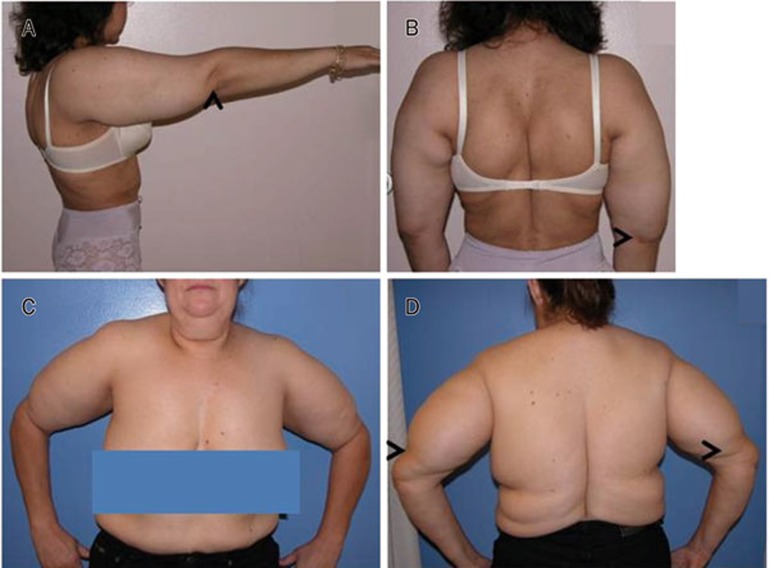
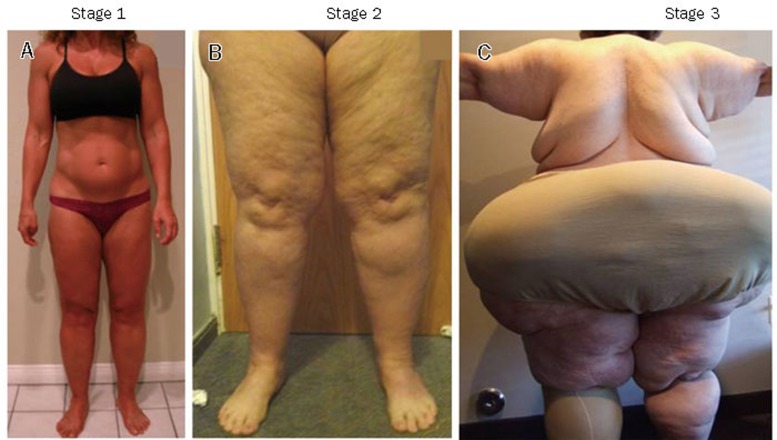
Rare adipose disorders (RADs) including multiple symmetric lipomatosis (MSL), lipedema and Dercum's disease (DD) may be misdiagnosed as obesity. Lifestyle changes, such as reduced caloric intake and increased physical activity are standard care for obesity. Although lifestyle changes and bariatric surgery work effectively for the obesity component of RADs, these treatments do not routinely reduce the abnormal subcutaneous adipose tissue (SAT) of RADs. RAD SAT likely results from the growth of a brown stem cell population with secondary lymphatic dysfunction in MSL, or by primary vascular and lymphatic dysfunction in lipedema and DD. People with RADs do not lose SAT from caloric limitation and increased energy expenditure alone. In order to improve recognition of RADs apart from obesity, the diagnostic criteria, histology and pathophysiology of RADs are presented and contrasted to familial partial lipodystrophies, acquired partial lipodystrophies and obesity with which they may be confused. Treatment recommendations focus on evidence-based data and include lymphatic decongestive therapy, medications and supplements that support loss of RAD SAT. Associated RAD conditions including depression, anxiety and pain will improve as healthcare providers learn to identify and adopt alternative treatment regimens for the abnormal SAT component of RADs. Effective dietary and exercise regimens are needed in RAD populations to improve quality of life and construct advanced treatment regimens for future generations.
Figures


References
-
- Ogden CL, Carroll MD.Prevalence of overweight, obesity, and extreme obesity among adults: united states, trends 1960–1962 through 2007–2008 . http://www.cdc.gov/nchs/fastats/overwt.htm .
-
- Orsi CM, Hale DE, Lynch JL. Pediatric obesity epidemiology. Curr Opin Endocrinol Diabetes Obes. 2011;18:14–22. - PubMed
-
- James WP, Caterson ID, Coutinho W, Finer N, Van Gaal LF, Maggioni AP, et al. Effect of sibutramine on cardiovascular outcomes in overweight and obese subjects. N Engl J Med. 2010;363:905–17. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
