

Diabetic retinopathy equity profile in a multi-ethnic, deprived population in Northern England
- PMID: 22302063
- PMCID: PMC3351065
- DOI: 10.1038/eye.2012.3
Diabetic retinopathy equity profile in a multi-ethnic, deprived population in Northern England
Abstract
Purpose: Equity profiles are an established public health tool used to systematically identify and address inequity within health and health services. Our aim was to conduct an equity profile to identify inequity in eye health across Leeds and Bradford. This paper presents results of findings for diabetic retinopathy in Bradford and Airedale.
Methods: A variety of routine health data were included and sub-analysed by measures of equity, including age, sex, ethnicity, and deprivation to identify inequity in eye health and healthcare. The Spearman Rank Correlation Coefficient was used to determine the association between variables.
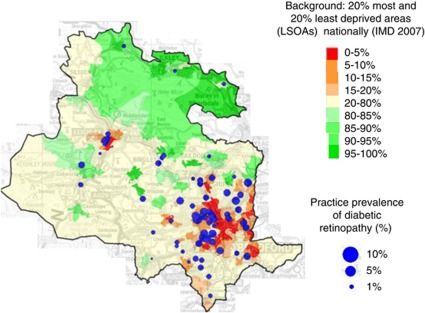
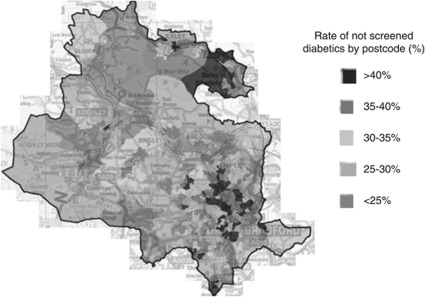
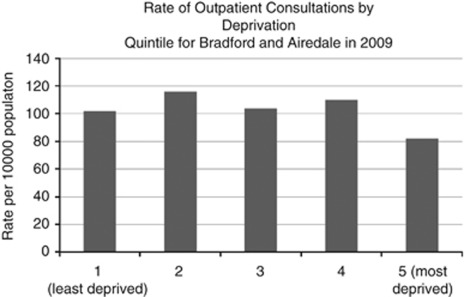
Results: The prevalence of diagnosed diabetes in Bradford and Airedale district is 6.6% compared to 4.3% in nearby Leeds and 5.1% nationally. The age-standardised prevalence of diagnosed diabetic retinopathy within Bradford and Airedale is 2.21% (95% CI 1.54-2.26%), with a disproportionately high prevalence of disease in the Pakistani population and the most deprived parts of the population. There was a poorer uptake of diabetic retinopathy screening in more deprived parts of the district and the proportions with a higher rate of referral to ophthalmology following the screening in Black and Minority Ethnic populations compared with the white population (13.2% vs 6.9%). Uptake of secondary care outpatient appointments is much lower in more deprived populations.
Conclusion: Inequalities are inherent in diabetic retinopathy prevalence, diagnosis, and treatment. The reasons for these inequities are multi-factorial and further investigation of reasons for poor uptake of services is required. Addressing the inequalities in eye health and healthcare requires cross-organisational collaboration.
Figures
References
-
- Bunce C, Wormald R. Causes of blind certifications in England and Wales: April 1999-March 2000. Eye. 2008;22 (7:905–911. - PubMed
-
- Diabetes UK Causes and Risk Factors 2010 . http://www.diabetes.org.uk/Guide-to-diabetes/Introduction-to-diabetes/Ca... (accessed 11 February 2010).
-
- Vision 2020 UK . UK Vision Strategy: Setting the Direction for Eye Health and Sight Loss Services. Vision 2020 UK: London; 2009.
-
- Department of Health . Health Equity Audit: A Guide for the NHS. Department of Health: London; 2003.
-
- NHS Bradford and Airedale & NHS Leeds Eye Health Equity Profile 2011 . http://www.observatory.bradford.nhs.uk/SiteCollectionDocuments/equity%20... (accessed 14 July 2011).
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
