

The relationship between femoral tunnels created by the transtibial, anteromedial portal, and outside-in techniques and the anterior cruciate ligament footprint
- PMID: 22302206
- PMCID: PMC3740359
- DOI: 10.1177/0363546511434276
The relationship between femoral tunnels created by the transtibial, anteromedial portal, and outside-in techniques and the anterior cruciate ligament footprint
Abstract
Background: Tunnels created for reconstruction of a torn anterior cruciate ligament (ACL) are critical determinants of joint stability and clinical outcomes. There is limited objective evidence on the ability of transtibial (TT), anteromedial (AM) portal, and outside-in (OI) operative techniques in creating anatomic tunnels.
Hypothesis: (1) Tibial tunnel-independent techniques can create tunnels more accurately at the anatomic ACL footprint center than the TT technique, and (2) femoral tunnel exit location of the OI and TT techniques on the lateral cortex will be significantly further away from the lateral epicondyle than the femoral tunnel exit location of the AM portal technique.
Study design: Controlled laboratory study.
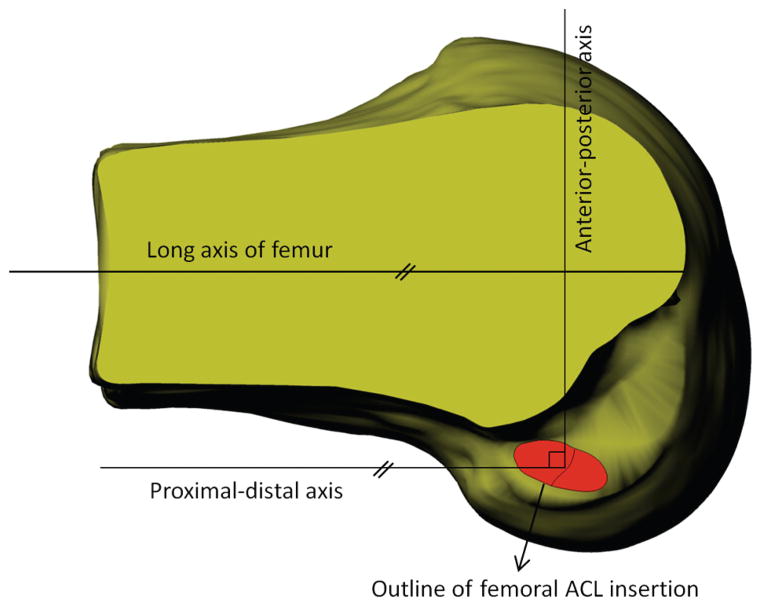
Methods: Eight cadaveric knee specimens with a mean age of 56 years were used in this study. A digitizing system was used to record points along the outlines of the ACL insertion area and apertures of tunnels created by the TT, AM portal, and OI techniques. The following parameters were measured from the digitized points: (1) amount of ACL, anteromedial bundle, and posterolateral bundle coverage by the tunnels; (2) relationship between the centers of the ACL and the tunnels; and (3) distance between the center of the femoral tunnel exit and the lateral epicondyle. All the recorded parameters were analyzed in 3-dimensional solid modeling software.
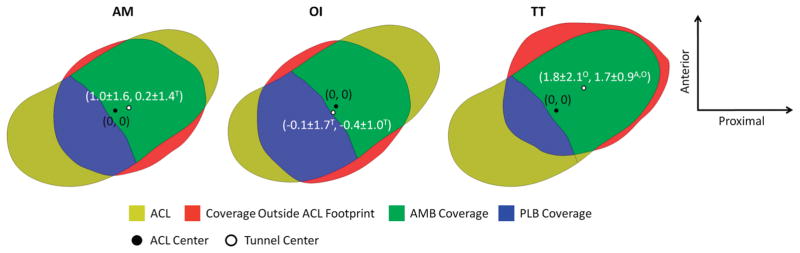
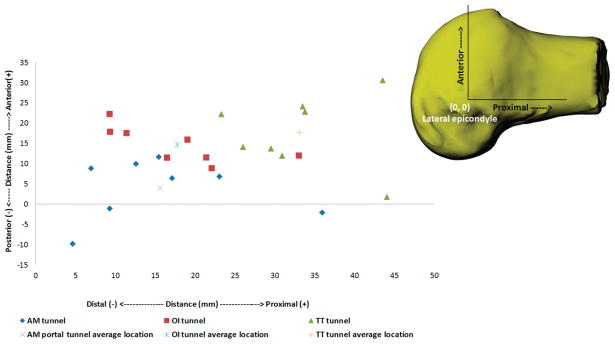
Results: The percentage of ACL footprint coverage achieved by all 3 surgical techniques was not significantly different from one another. However, larger femoral posterolateral bundle coverage was observed in tunnels created by the AM portal and OI techniques than in the TT tunnel. In terms of anteromedial bundle coverage, no significant differences were observed between the 3 techniques. On average, 27.1% ± 17.4% of the TT tunnel was outside the ACL footprint. This was significantly larger compared with 13.6% ± 15.7% with the AM portal technique (P = .01) and 10.8% ± 10.8% in the OI technique (P = .01). Centers of femoral tunnels created by the TT, AM portal, and OI techniques were located at a distance of 3.0 ± 1.5 mm, 2.1 ± 0.9 mm, and 1.5 ± 1.2 mm, respectively, from the ACL footprint center. The femoral tunnel exit location of the AM portal technique on the lateral femoral cortex was closer to the lateral epicondyle than the femoral tunnel exit location of the OI and TT techniques.
Conclusion: Findings of this study indicate that a larger posterolateral bundle coverage is achieved by the AM portal and OI techniques than by the TT technique. Centers of the tunnels created by the AM portal and OI techniques were closer to the native ACL footprint center than the center of the TT technique tunnel. The incidence of a posterior femoral tunnel exit relative to the lateral epicondyle is higher in the AM portal technique than in the OI and TT techniques.
Clinical relevance: For ACL reconstruction using soft tissue grafts, tibial tunnel-independent techniques can produce more anatomic tunnels than the TT technique.
Figures

References
-
- Abebe ES, Moorman CT, 3rd, Dziedzic TS, et al. Femoral tunnel placement during anterior cruciate ligament reconstruction: an in vivo imaging analysis comparing transtibial and 2-incision tibial tunnel-independent techniques. Am J Sports Med. 2009;37(10):1904–1911. - PubMed
-
- Behrendt S, Richter J. Anterior cruciate ligament reconstruction: drilling a femoral posterolateral tunnel cannot be accomplished using an over-the-top step-off drill guide. Knee Surg Sports Traumatol Arthrosc. 2010;18(9):1252–1256. - PubMed
-
- Duquin TR, Wind WM, Fineberg MS, Smolinski RJ, Buyea CM. Current trends in anterior cruciate ligament reconstruction. J Knee Surg. 2009;22(1):7–12. - PubMed
-
- Farrow LD, Parker RD. The relationship of lateral anatomic structures to exiting guide pins during femoral tunnel preparation utilizing an accessory medial portal. Knee Surg Sports Traumatol Arthrosc. 2010;18(6):747–753. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
