

Serologic diagnosis of NMO: a multicenter comparison of aquaporin-4-IgG assays
- PMID: 22302543
- PMCID: PMC3286228
- DOI: 10.1212/WNL.0b013e318248dec1
Serologic diagnosis of NMO: a multicenter comparison of aquaporin-4-IgG assays
Abstract
Objectives: Neuromyelitis optica (NMO) immunoglobulin G (IgG) (aquaporin-4 [AQP4] IgG) is highly specific for NMO and related disorders, and autoantibody detection has become an essential investigation in patients with demyelinating disease. However, although different techniques are now used, no multicenter comparisons have been performed. This study compares the sensitivity and specificity of different assays, including an in-house flow cytometric assay and 2 commercial assays (ELISA and transfected cell-based assay [CBA]).
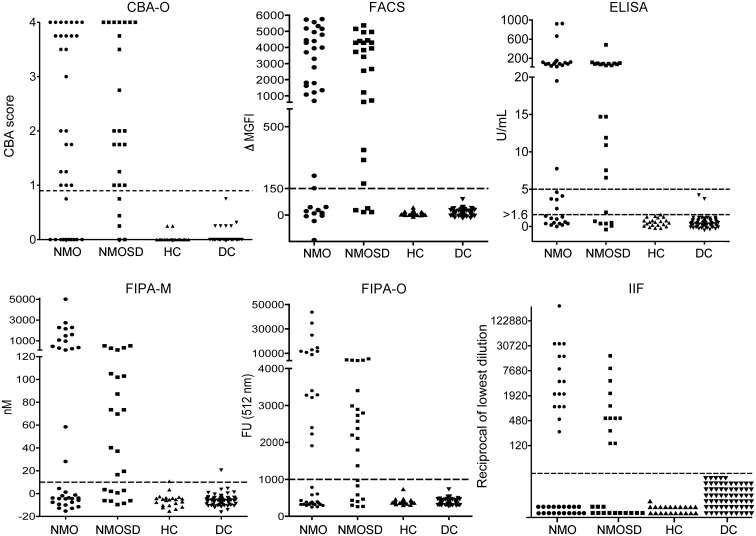
Methods: Six assay methods (in-house or commercial) were performed in 2 international centers using coded serum from patients with NMO (35 patients), NMO spectrum disorders (25 patients), relapsing-remitting multiple sclerosis (39 patients), miscellaneous autoimmune diseases (25 patients), and healthy subjects (22 subjects).
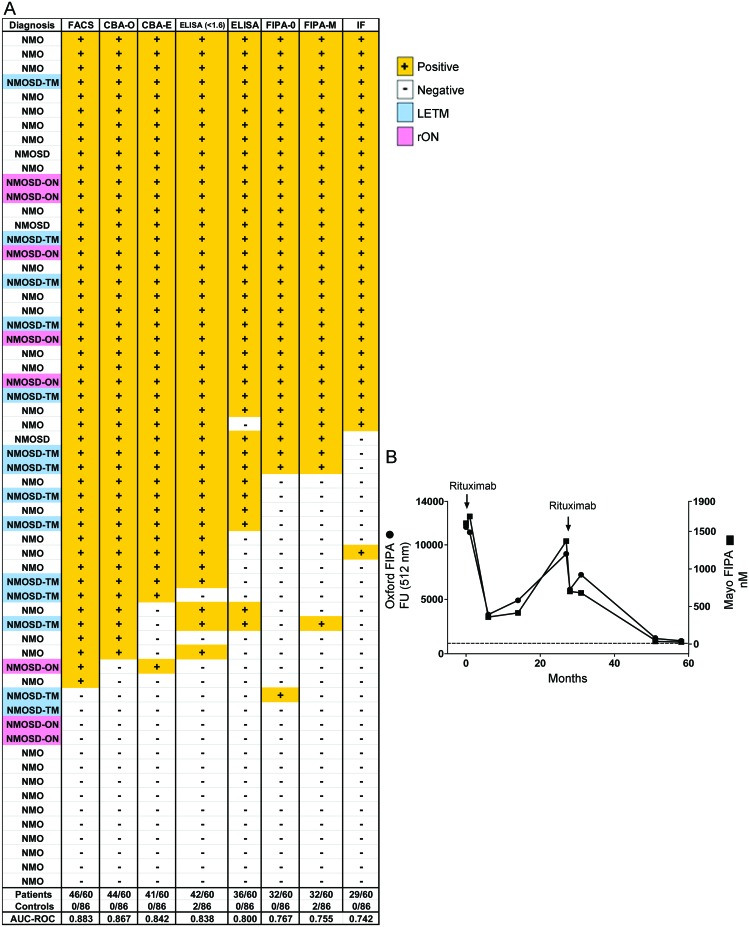
Results: The highest sensitivities were yielded by assays detecting IgG binding to cells expressing recombinant AQP4 with quantitative flow cytometry (77; 46 of 60) or visual observation (CBA, 73%; 44 of 60). The fluorescence immunoprecipitation assay and tissue-based immunofluorescence assay were least sensitive (48%-53%). The CBA and ELISA commercial assays (100% specific) yielded sensitivities of 68% (41 of 60) and 60% (36 of 60), respectively, and sensitivity of 72% (43 of 60) when used in combination.
Conclusions: The greater sensitivity and excellent specificity of second-generation recombinant antigen-based assays for detection of NMO-IgG in a clinical setting should enable earlier diagnosis of NMO spectrum disorders and prompt initiation of disease-appropriate therapies.
Figures
References
-
- Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG. The spectrum of neuromyelitis optica. Lancet Neurol 2007;6:805–815 - PubMed
-
- Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica. Neurology 2006;66:1485–1489 - PubMed
-
- Lennon VA, Wingerchuk DM, Kryzer TJ, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet 2004;364:2106–2112 - PubMed
-
- Hinson SR, Pittock SJ, Lucchinetti CF, et al. Pathogenic potential of IgG binding to water channel extracellular domain in neuromyelitis optica. Neurology 2007;69:2221–2231 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources