

Effectiveness of multifaceted educational programme to reduce antibiotic dispensing in primary care: practice based randomised controlled trial
- PMID: 22302780
- PMCID: PMC3270575
- DOI: 10.1136/bmj.d8173
Effectiveness of multifaceted educational programme to reduce antibiotic dispensing in primary care: practice based randomised controlled trial
Abstract
Objective: To evaluate the effectiveness and costs of a multifaceted flexible educational programme aimed at reducing antibiotic dispensing at the practice level in primary care.
Design: Randomised controlled trial with general practices as the unit of randomisation and analysis. Clinicians and researchers were blinded to group allocation until after randomisation.
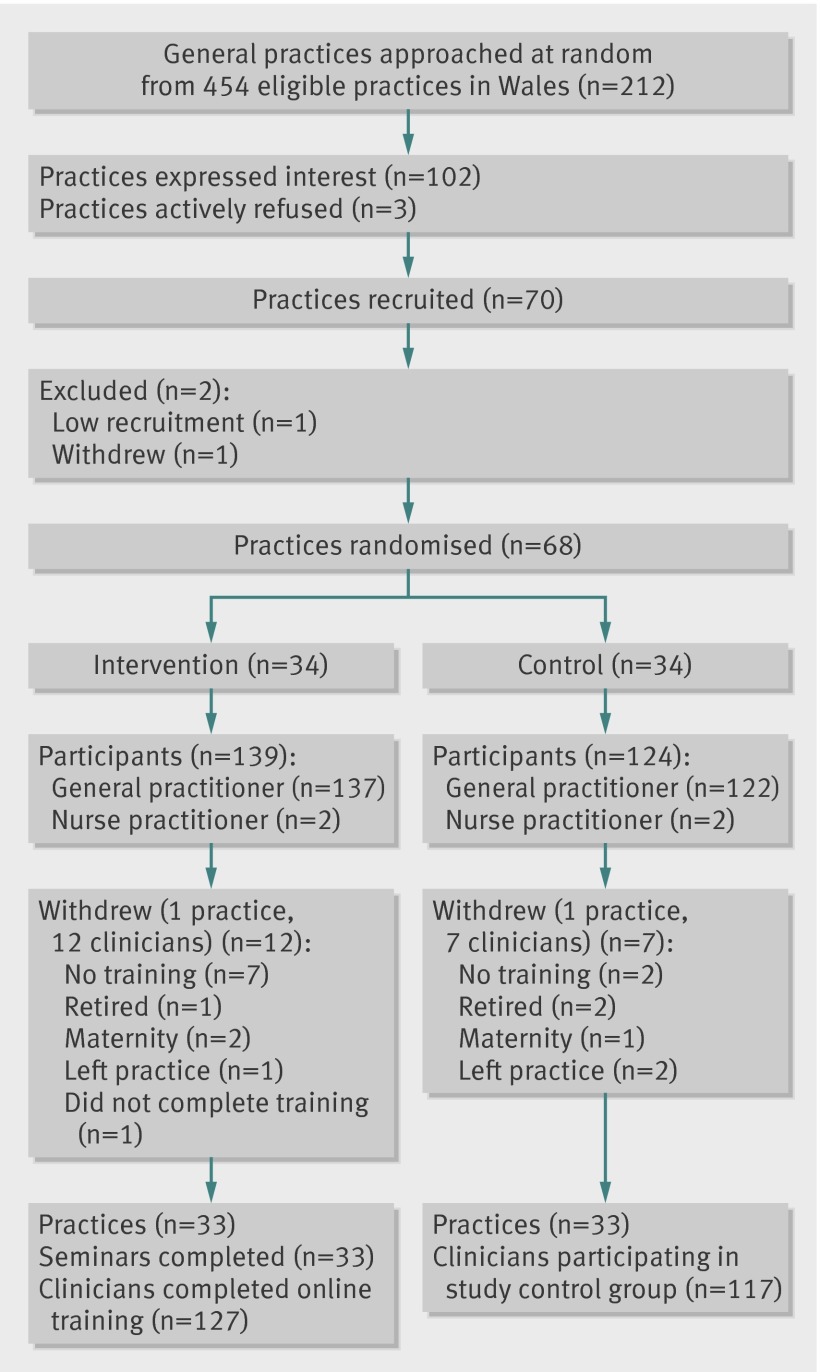
Setting: 68 general practices with about 480,000 patients in Wales, United Kingdom.
Participants: 34 practices were randomised to receive the educational programme and 34 practices to be controls. 139 clinicians from the intervention practices and 124 from control practices had agreed to participate before randomisation. Practice level data covering all the clinicians in the 68 practices were analysed.
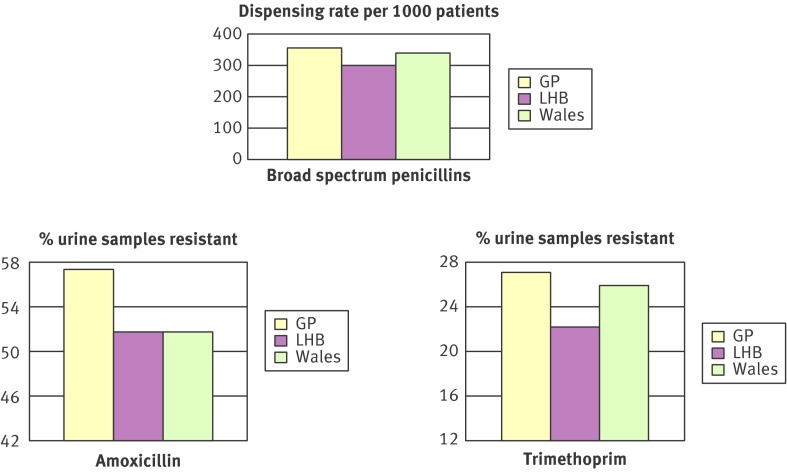
Interventions: Intervention practices followed the Stemming the Tide of Antibiotic Resistance (STAR) educational programme, which included a practice based seminar reflecting on the practices' own dispensing and resistance data, online educational elements, and practising consulting skills in routine care. Control practices provided usual care.
Main outcome measures: Total numbers of oral antibiotic items dispensed for all causes per 1000 practice patients in the year after the intervention, adjusted for the previous year's dispensing. Secondary outcomes included reconsultations, admissions to hospital for selected causes, and costs.
Results: The rate of oral antibiotic dispensing (items per 1000 registered patients) decreased by 14.1 in the intervention group but increased by 12.1 in the control group, a net difference of 26.1. After adjustment for baseline dispensing rate, this amounted to a 4.2% (95% confidence interval 0.6% to 7.7%) reduction in total oral antibiotic dispensing for the year in the intervention group relative to the control group (P=0.02). Reductions were found for all classes of antibiotics other than penicillinase-resistant penicillins but were largest and significant individually for phenoxymethylpenicillins (penicillin V) (7.3%, 0.4% to 13.7%) and macrolides (7.7%, 1.1% to 13.8%). There were no significant differences between intervention and control practices in the number of admissions to hospital or in reconsultations for a respiratory tract infection within seven days of an index consultation. The mean cost of the programme was £2923 (€3491, $4572) per practice (SD £1187). There was a 5.5% reduction in the cost of dispensed antibiotics in the intervention group compared with the control group (-0.4% to 11.4%), equivalent to a reduction of about £830 a year for an average intervention practice.
Conclusion: The STAR educational programme led to reductions in all cause oral antibiotic dispensing over the subsequent year with no significant change in admissions to hospital, reconsultations, or costs. Trial registration ISRCT No 63355948.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
A prescription for improving antibiotic prescribing in primary care.BMJ. 2012 Feb 2;344:d7955. doi: 10.1136/bmj.d7955. BMJ. 2012. PMID: 22302779 No abstract available.
-
[Education of physicians: necessary but not sufficient to decrease antibiotic prescription].Med Mal Infect. 2012 May;42(5):237-8. doi: 10.1016/j.medmal.2012.03.002. Med Mal Infect. 2012. PMID: 22844679 French. No abstract available.
References
-
- Goossens H, Ferech M, Vander Stichele R, Elseviers M. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet 2005;365:579-87. - PubMed
-
- Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ 2010;340:c2096. - PubMed
-
- Glasziou P, del Mar C, Sanders S, Hayem M. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev 2004;1:CD000219. - PubMed
-
- Del Mar CB, Glasziou PP, Spinks AB. Antibiotics for sore throat. Cochrane Database Syst Rev 2006;4:CD000023. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical