

High-resolution genotyping of the endemic Salmonella Typhi population during a Vi (typhoid) vaccination trial in Kolkata
- PMID: 22303491
- PMCID: PMC3269425
- DOI: 10.1371/journal.pntd.0001490
High-resolution genotyping of the endemic Salmonella Typhi population during a Vi (typhoid) vaccination trial in Kolkata
Abstract
Background: Typhoid fever, caused by Salmonella enterica serovar Typhi (S. Typhi), is a major health problem especially in developing countries. Vaccines against typhoid are commonly used by travelers but less so by residents of endemic areas.
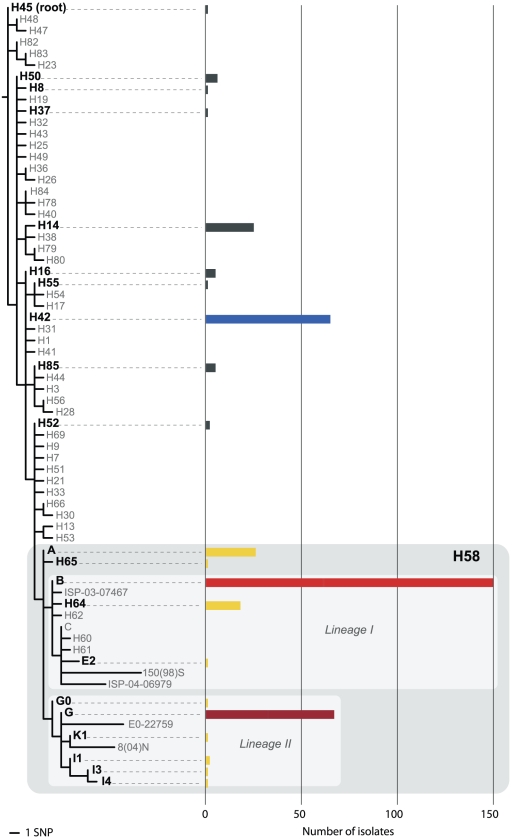
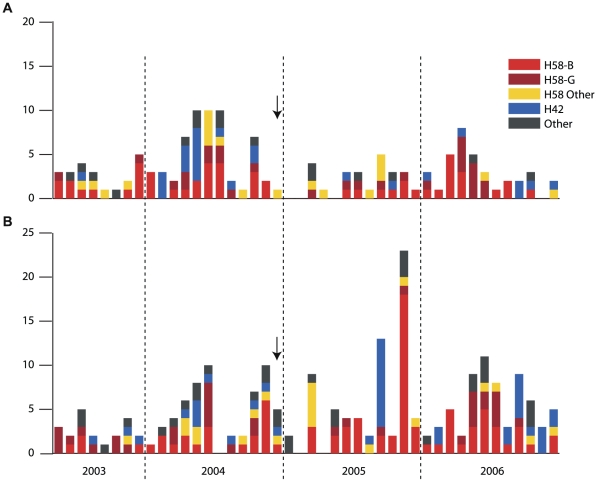
Methodology: We used single nucleotide polymorphism (SNP) typing to investigate the population structure of 372 S. Typhi isolated during a typhoid disease burden study and Vi vaccine trial in Kolkata, India. Approximately sixty thousand people were enrolled for fever surveillance for 19 months prior to, and 24 months following, Vi vaccination of one third of the study population (May 2003-December 2006, vaccinations given December 2004).
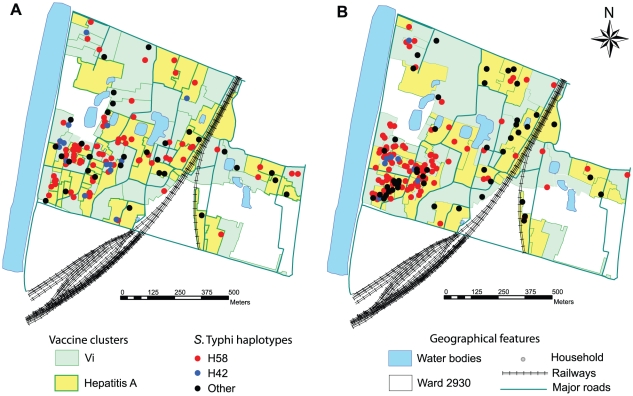
Principal findings: A diverse S. Typhi population was detected, including 21 haplotypes. The most common were of the H58 haplogroup (69%), which included all multidrug resistant isolates (defined as resistance to chloramphenicol, ampicillin and co-trimoxazole). Quinolone resistance was particularly high among H58-G isolates (97% Nalidixic acid resistant, 30% with reduced susceptibility to ciprofloxacin). Multiple typhoid fever episodes were detected in 22 households, however household clustering was not associated with specific S. Typhi haplotypes.
Conclusions: Typhoid fever in Kolkata is caused by a diverse population of S. Typhi, however H58 haplotypes dominate and are associated with multidrug and quinolone resistance. Vi vaccination did not obviously impact on the haplotype population structure of the S. Typhi circulating during the study period.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Temporal fluctuation of multidrug resistant salmonella typhi haplotypes in the mekong river delta region of Vietnam.PLoS Negl Trop Dis. 2011 Jan 4;5(1):e929. doi: 10.1371/journal.pntd.0000929. PLoS Negl Trop Dis. 2011. PMID: 21245916 Free PMC article. Clinical Trial.
-
Antimicrobial resistance and molecular subtypes of Salmonella enterica serovar Typhi isolates from Kolkata, India over a 15 years period 1998-2012.Int J Med Microbiol. 2017 Jan;307(1):28-36. doi: 10.1016/j.ijmm.2016.11.006. Epub 2016 Nov 25. Int J Med Microbiol. 2017. PMID: 27916384
-
Laboratory characterisation of Salmonella enterica serotype Typhi isolates from Zimbabwe, 2009-2017.BMC Infect Dis. 2019 May 31;19(1):487. doi: 10.1186/s12879-019-4114-0. BMC Infect Dis. 2019. PMID: 31151421 Free PMC article.
-
Assessing Salmonella Typhi Pathogenicity and Prevention: The Crucial Role of Vaccination in Combating Typhoid Fever.Int J Mol Sci. 2025 Apr 23;26(9):3981. doi: 10.3390/ijms26093981. Int J Mol Sci. 2025. PMID: 40362220 Free PMC article. Review.
-
Review of current typhoid fever vaccines, cross-protection against paratyphoid fever, and the European guidelines.Expert Rev Vaccines. 2017 Oct;16(10):1029-1043. doi: 10.1080/14760584.2017.1374861. Expert Rev Vaccines. 2017. PMID: 28856924 Review.
Cited by
-
Spatial-temporal and phylogenetic analyses of epidemiologic data to help understand the modes of transmission of endemic typhoid fever in Samoa.PLoS Negl Trop Dis. 2022 Oct 17;16(10):e0010348. doi: 10.1371/journal.pntd.0010348. eCollection 2022 Oct. PLoS Negl Trop Dis. 2022. PMID: 36251704 Free PMC article.
-
Non-typhoidal Salmonella gastroenteritis at a diarrheal hospital in Dhaka, Bangladesh, 1996-2011.Am J Trop Med Hyg. 2013 Apr;88(4):661-9. doi: 10.4269/ajtmh.12-0672. Epub 2013 Jan 28. Am J Trop Med Hyg. 2013. PMID: 23358644 Free PMC article.
-
Non-specificity of sequence characterised amplified region as an alternative molecular epidemiology marker for the identification of Salmonella enterica subspecies enterica serovar Typhi.BMC Res Notes. 2018 Oct 29;11(1):766. doi: 10.1186/s13104-018-3870-z. BMC Res Notes. 2018. PMID: 30373642 Free PMC article.
-
Genome-wide SNP-genotyping array to study the evolution of the human pathogen Vibrio vulnificus biotype 3.PLoS One. 2014 Dec 19;9(12):e114576. doi: 10.1371/journal.pone.0114576. eCollection 2014. PLoS One. 2014. PMID: 25526263 Free PMC article.
-
MinION nanopore sequencing identifies the position and structure of a bacterial antibiotic resistance island.Nat Biotechnol. 2015 Mar;33(3):296-300. doi: 10.1038/nbt.3103. Epub 2014 Dec 8. Nat Biotechnol. 2015. PMID: 25485618
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
