

Staging and comorbidities
- PMID: 22303751
- PMCID: PMC3997993
- DOI: 10.1055/s-0031-1297362
Staging and comorbidities
Abstract
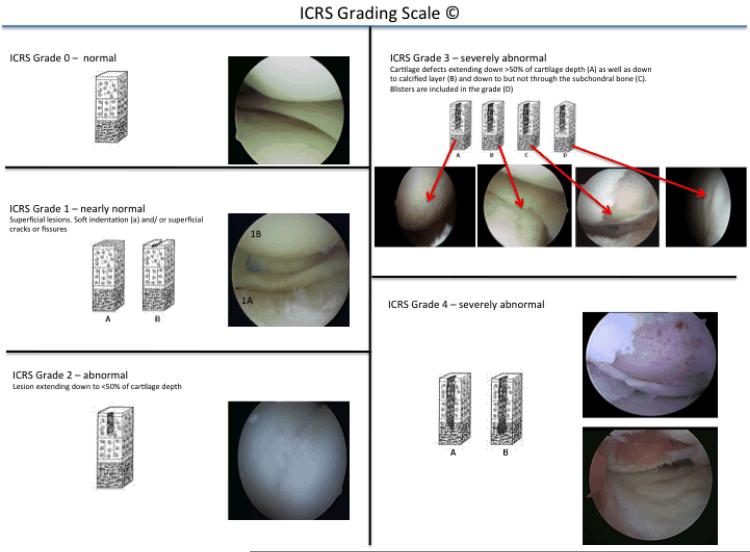
Articular cartilage lesions of the distal femur and patella are common. To provide an accurate diagnosis of a clinically symptomatic cartilage lesion and subsequent appropriate planning for potential treatment options, a proper staging is required. This includes clinical exam, radiographic imaging as well as arthroscopy. Once the staging is completed, other comorbidities may need to be addressed that may require additional surgical procedures. These can either be planned as staged procedures or concomitantly with a cartilage repair procedure. This article will discuss this staging and evaluation process in depth to serve as a guideline to the orthopaedic surgeon engaged in the treatment of cartilage defects in patients with early posttraumatic osteoarthritis (OA).
Figures

References
-
- Hjelle K, Solheim E, Strand T, Muri R, Brittberg M. Articular cartilage defects in 1,000 knee arthroscopies. Arthroscopy. 2002 Sep;18(7):730–734. - PubMed
-
- Widuchowski W, Lukasik P, Kwiatkowski G, et al. Isolated full thickness chondral injuries. Prevalance and outcome of treatment. A retrospective study of 5233 knee arthroscopies. Acta Chir Orthop Traumatol Cech. 2008 Oct;75(5):382–386. - PubMed
-
- Curl WW, Krome J, Gordon ES, Rushing J, Smith BP, Poehling GG. Cartilage injuries: a review of 31,516 knee arthroscopies. Arthroscopy. 1997 Aug;13(4):456–460. - PubMed
-
- Widuchowski W, Widuchowski J, Faltus R, et al. Long-term clinical and radiological assessment of untreated severe cartilage damage in the knee: a natural history study. Scand J Med Sci Sports. 2011 Feb;21(1):106–110. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical