

Predictors of warfarin use in atrial fibrillation in the United States: a systematic review and meta-analysis
- PMID: 22304704
- PMCID: PMC3395868
- DOI: 10.1186/1471-2296-13-5
Predictors of warfarin use in atrial fibrillation in the United States: a systematic review and meta-analysis
Abstract
Background: Despite warfarin's marked efficacy, not all eligible patients receive it for stroke prevention in AF. The aim of this meta-analysis was to evaluate the association between prescriber and/or patient characteristics and subsequent prescription of warfarin for stroke prevention in patients with atrial fibrillation (AF).
Methods: Observational studies conducted in the US using multivariate analysis to determine the relationship between characteristics and the odds of receiving warfarin for stroke prevention were identified in MEDLINE, EMBASE and a manual review of references. Effect estimates of prescriber and/or patient characteristics from individual studies were pooled to calculate odds ratios (ORs) with 95% confidence intervals.
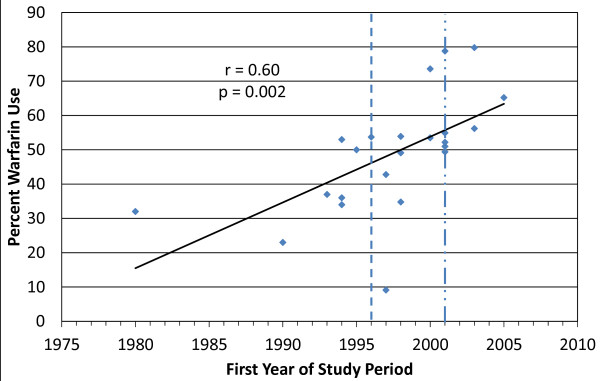
Results: Twenty-eight studies reporting results of 33 unique multivariate analyses were identified. Warfarin use across studies ranged from 9.1%-79.8% (median=49.1%). There was a moderately-strong correlation between warfarin use and year of study (r=0.60, p=0.002). Upon meta-analysis, characteristics associated with a statistically significant increase in the odds of warfarin use included history of cerebrovascular accident (OR=1.59), heart failure (OR=1.36), and male gender (OR=1.12). Those associated with a significant reduction in the odds of warfarin use included alcohol/drug abuse (OR=0.62), perceived barriers to compliance (OR=0.87), contraindication(s) to warfarin (OR=0.81), dementia (OR=0.32), falls (OR=0.60), gastrointestinal hemorrhage (OR=0.47), intracranial hemorrhage (OR=0.39), hepatic (OR=0.59), and renal impairment (OR=0.69). While age per 10-year increase (OR=0.78) and advancing age as a dichotomized variable (cut-off varied by study) (OR=0.57) were associated with significant reductions in warfarin use; qualitative review of results of studies evaluating age as a categorical variable did not confirm this relationship.
Conclusions: Warfarin use has increased somewhat over time. The decision to prescribe warfarin for stroke prevention in atrial fibrillation is based upon multiple prescriber and patient characteristics. These findings can be used by family practice prescribers and other healthcare decision-makers to target interventions or methods to improve utilization of warfarin when it is indicated for stroke prevention.
Figures
Similar articles
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Direct oral anticoagulants versus warfarin for preventing stroke and systemic embolic events among atrial fibrillation patients with chronic kidney disease.Cochrane Database Syst Rev. 2017 Nov 6;11(11):CD011373. doi: 10.1002/14651858.CD011373.pub2. Cochrane Database Syst Rev. 2017. PMID: 29105079 Free PMC article.
-
Warfarin and the Risk of Stroke and Bleeding in Patients With Atrial Fibrillation Receiving Dialysis: A Systematic Review and Meta-analysis.Can J Cardiol. 2017 Jun;33(6):737-746. doi: 10.1016/j.cjca.2017.02.004. Epub 2017 Feb 20. Can J Cardiol. 2017. PMID: 28545622
-
WITHDRAWN: Anticoagulants or antiplatelet therapy for non-rheumatic atrial fibrillation and flutter.Cochrane Database Syst Rev. 2007 Jul 18;2006(3):CD001938. doi: 10.1002/14651858.CD001938.pub2. Cochrane Database Syst Rev. 2007. PMID: 17636690 Free PMC article.
-
Anticoagulants or antiplatelet therapy for non-rheumatic atrial fibrillation and flutter.Cochrane Database Syst Rev. 2001;(1):CD001938. doi: 10.1002/14651858.CD001938. Cochrane Database Syst Rev. 2001. Update in: Cochrane Database Syst Rev. 2007 Jul 18;(3):CD001938. doi: 10.1002/14651858.CD001938.pub2. PMID: 11279741 Updated.
Cited by
-
Cost-Effectiveness of Novel Oral Anticoagulants for Stroke Prevention in Non-Valvular Atrial Fibrillation.Curr Cardiol Rep. 2015 Aug;17(8):61. doi: 10.1007/s11886-015-0618-4. Curr Cardiol Rep. 2015. PMID: 26081245 Review.
-
Time trends in antithrombotic therapy prescription patterns: Real-world monocentric study in hospitalized patients with atrial fibrillation.World J Cardiol. 2022 Nov 26;14(11):576-598. doi: 10.4330/wjc.v14.i11.576. World J Cardiol. 2022. PMID: 36483763 Free PMC article.
-
Heart disease and stroke statistics--2013 update: a report from the American Heart Association.Circulation. 2013 Jan 1;127(1):e6-e245. doi: 10.1161/CIR.0b013e31828124ad. Epub 2012 Dec 12. Circulation. 2013. PMID: 23239837 Free PMC article. Review. No abstract available.
-
Effectiveness and Safety of Apixaban, Dabigatran, and Rivaroxaban Versus Warfarin in Frail Patients With Nonvalvular Atrial Fibrillation.J Am Heart Assoc. 2018 Apr 13;7(8):e008643. doi: 10.1161/JAHA.118.008643. J Am Heart Assoc. 2018. PMID: 29654196 Free PMC article.
-
Influence of Age on Warfarin Dose, Anticoagulation Control, and Risk of Hemorrhage.Pharmacotherapy. 2018 Jun;38(6):588-596. doi: 10.1002/phar.2089. Epub 2018 Feb 27. Pharmacotherapy. 2018. PMID: 29393514 Free PMC article.
References
-
- Go AS, Hylek EM, Phillips KA. et al.Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–2375. doi: 10.1001/jama.285.18.2370. - DOI - PubMed
-
- Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation: analysis of pooled data from five randomized controlled trials. Arch Intern Med. 1994;154:1449–1457. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
