

Prehospital trauma care reduces mortality. Ten-year results from a time-cohort and trauma audit study in Iraq
- PMID: 22304808
- PMCID: PMC3298775
- DOI: 10.1186/1757-7241-20-13
Prehospital trauma care reduces mortality. Ten-year results from a time-cohort and trauma audit study in Iraq
Abstract
Background: Blunt implementation of Western trauma system models is not feasible in low-resource communities with long prehospital transit times. The aims of the study were to evaluate to which extent a low-cost prehospital trauma system reduces trauma deaths where prehospital transit times are long, and to identify specific life support interventions that contributed to survival.
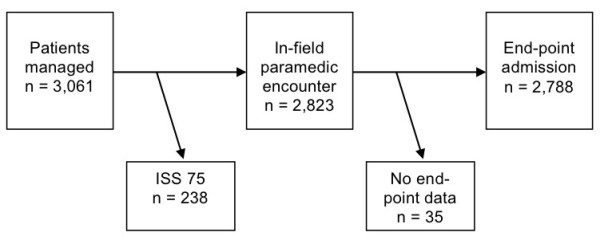
Methods: In the study period from 1997 to 2006, 2,788 patients injured by land mines, war, and traffic accidents were managed by a chain-of-survival trauma system where non-graduate paramedics were the key care providers. The study was conducted with a time-period cohort design.
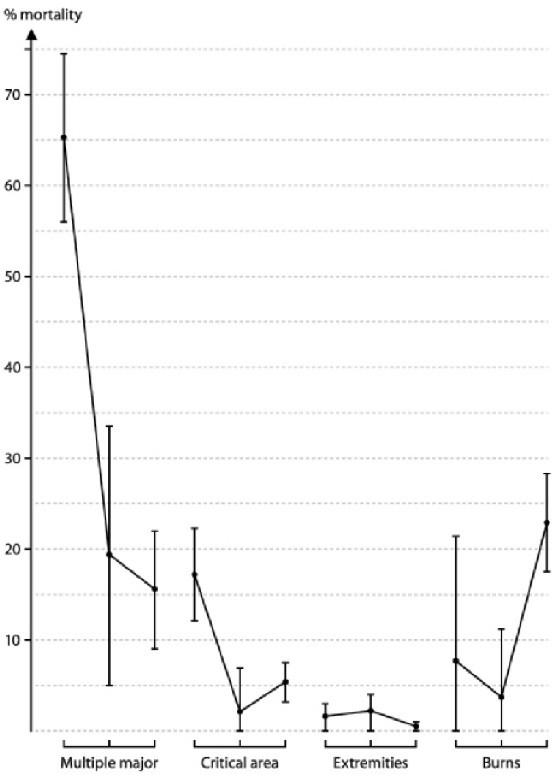
Results: 37% of the study patients had serious injuries with Injury Severity Score ≥ 9. The mean prehospital transport time was 2.5 hours (95% CI 1.9 - 3.2). During the ten-year study period trauma mortality was reduced from 17% (95% CI 15 -19) to 4% (95% CI 3.5 - 5), survival especially improving in major trauma victims. In most patients with airway problems, in chest injured, and in patients with external hemorrhage, simple life support measures were sufficient to improve physiological severity indicators.
Conclusion: In case of long prehospital transit times simple life support measures by paramedics and lay first responders reduce trauma mortality in major injuries. Delegating life-saving skills to paramedics and lay people is a key factor for efficient prehospital trauma systems in low-resource communities.
Figures

References
-
- Mathers CD, Joncar D. Updated projections of global mortality and burden of disease, 2002 - 2030: data sources, methods, and results. http://www.who.int/healthinfo/statistics/bod_projections2030_-paper.pdf accessed 30/10/2011. - PMC - PubMed
-
- Jahanlu HR, Husum H, Wisborg T. Mortality in landmine accidents in Iran. Prehosp Disast Med. 2002;17:107–9. - PubMed
-
- Husum H, Gilbert M, Wisborg T. Save Lives, Save Limbs. Life support to victims of mines, wars, and accidents. Penang, Malaysia: Third World Network; 2000.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
