

Heavy smoking during pregnancy as a marker for other risk factors of adverse birth outcomes: a population-based study in British Columbia, Canada
- PMID: 22304990
- PMCID: PMC3339515
- DOI: 10.1186/1471-2458-12-102
Heavy smoking during pregnancy as a marker for other risk factors of adverse birth outcomes: a population-based study in British Columbia, Canada
Abstract
Background: Smoking during pregnancy is associated with known adverse perinatal and obstetrical outcomes as well as with socio-economic, demographic and other behavioural risk factors that independently influence outcomes. Using a large population-based perinatal registry, we assess the quantity of cigarettes smoked for the magnitude of adverse birth outcomes and also the association of other socio-economic and behavioural risk factors documented within the registry that influence pregnancy outcomes. Our goal was to determine whether number of cigarettes smoked could identify those in greatest need for comprehensive intervention programs to improve outcomes.
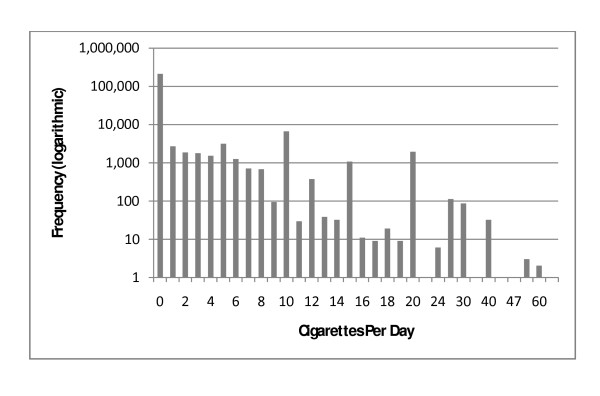
Methods: Our population-based retrospective study of singleton births from 2001 to 2006 (N = 237,470) utilized data obtained from the BC Perinatal Database Registry. Smoking data, self reported at the earliest prenatal visit, was categorized as: never, former, light (1 to 4), moderate (5 to 9), or heavy smoker (10 or more per day). Crude and adjusted odds ratios (AOR) with 95% confidence intervals (95% CI) were calculated using logistic regression models for smoking frequency and adverse birth outcomes. A partial proportional odds (pp-odds) model was used to determine the association between smoking status and other risk factors.
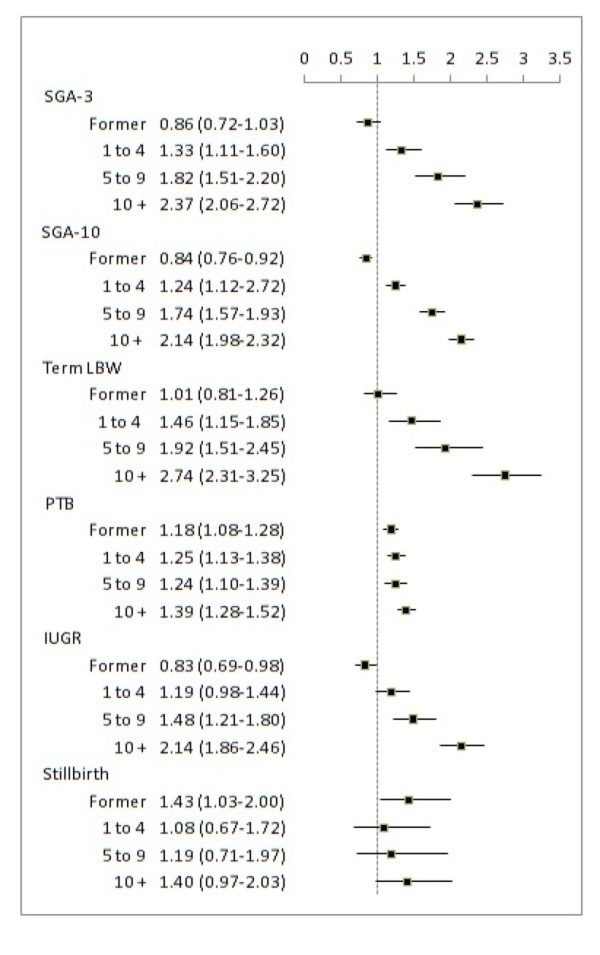
Results: There were 233,891 singleton births with available smoking status data. A significant dose-dependent increase in risk was observed for the adverse birth outcomes small-for-gestational age, term low birth weight and intra-uterine growth restriction. Results from the pp-odds model indicate heavy smokers were more likely to have not graduated high school: AOR (95% CI) = 3.80 (3.41-4.25); be a single parent: 2.27 (2.14-2.42); have indication of drug or alcohol use: 7.65 (6.99-8.39) and 2.20 (1.88-2.59) respectively, attend fewer than 4 prenatal care visits: 1.39 (1.23-1.58), and be multiparous: 1.59 (1.51-1.68) compared to light, moderate and non-smokers combined.
Conclusion: Our data suggests that self reports of heavy smoking early in pregnancy could be used as a marker for lifestyle risk factors that in combination with smoking influence birth outcomes. This information may be used for planning targeted intervention programs for not only smoking cessation, but potentially other support services such as nutrition and healthy pregnancy education.
Figures
References
-
- US Department of Health and Human Services. How tobacco smoke causes disease: the biology and behavioural basis for smoking-attributable disease: a report of the surgeon general. Atlanta GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office of Smoking and Health. 2010.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
