

Novel markers of kidney function as predictors of ESRD, cardiovascular disease, and mortality in the general population
- PMID: 22305758
- PMCID: PMC3880682
- DOI: 10.1053/j.ajkd.2011.11.042
Novel markers of kidney function as predictors of ESRD, cardiovascular disease, and mortality in the general population
Abstract
Background: Cystatin C level predicts mortality more strongly than serum creatinine level. It is unknown whether this advantage extends to other outcomes, such as kidney failure, or whether other novel renal filtration markers share this advantage in predicting outcomes.
Study design: Observational cohort study.
Setting & participants: 9,988 participants in the Atherosclerosis Risk in Communities (ARIC) Study, a population-based study in 4 US communities, followed for approximately 10 years.
Predictors: Serum creatinine-based estimated glomerular filtration rate calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation (eGFR(CKD-EPI)) and cystatin C, β-trace protein (BTP), and β(2)-microglobulin (B2M) levels.
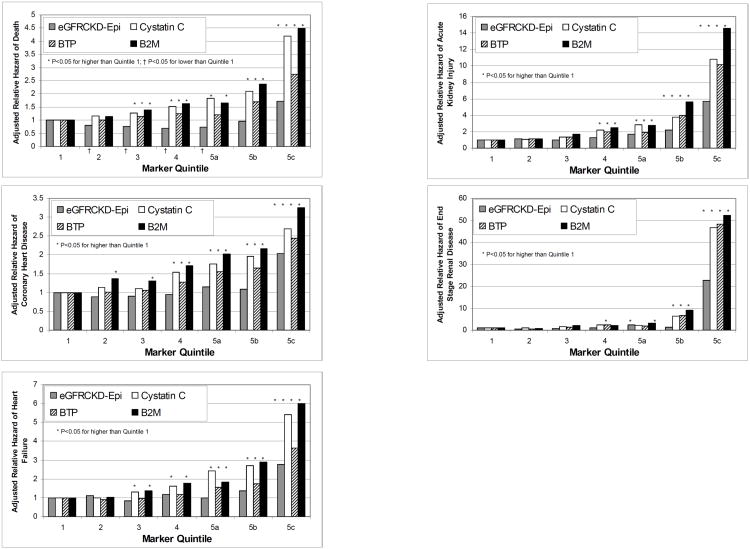
Outcomes: Mortality, coronary heart disease, heart failure, and kidney failure.
Results: Higher cystatin C and B2M concentrations were associated more strongly with mortality (n = 1,425) than BTP level and all were associated more strongly than eGFR(CKD-EPI) (adjusted HR for the upper 6.7 percentile compared with the lowest quintile: 1.6 [95% CI, 1.3-1.9] for eGFR(CKD-EPI), 2.9 [95% CI, 2.3-3.6] for cystatin C level, 1.9 [95% CI, 1.5-2.4] for BTP level, and 3.0 [95% CI, 2.4-3.8] for B2M level). Similar patterns were observed for coronary heart disease (n = 1,279), heart failure (n = 803), and kidney failure (n = 130). The addition of cystatin C, BTP, and B2M levels to models including eGFR(CKD-EPI) and all covariates, including urinary albumin-creatinine ratio, significantly improved risk prediction for all outcomes (P < 0.001).
Limitations: No direct measurement of GFR.
Conclusions: B2M and, to a lesser extent, BTP levels share cystatin C's advantage over eGFR(CKD-EPI) in predicting outcomes, including kidney failure. These additional markers may be helpful in improving estimation of risk associated with decreased kidney function beyond current estimates based on eGFR(CKD-EPI).
Copyright © 2012 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest.
Figures
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–1305. - PubMed
-
- Bash LD, Astor BC, Coresh J. Risk of incident ESRD: a comprehensive look at cardiovascular risk factors and 17 years of follow-up in the Atherosclerosis Risk in Communities (ARIC) Study. Am J Kidney Dis. 2010;55(1):31–41. - PubMed
-
- Shlipak MG, Sarnak MJ, Katz R, et al. Cystatin C and the risk of death and cardiovascular events among elderly persons. N Engl J Med. 2005;352(20):2049–2060. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC055022/HC/NHLBI NIH HHS/United States
- K23 DK083514/DK/NIDDK NIH HHS/United States
- N01-HC-55022/HC/NHLBI NIH HHS/United States
- N01-HC-55016/HC/NHLBI NIH HHS/United States
- N01 HC055018/HC/NHLBI NIH HHS/United States
- N01-HC-55021/HC/NHLBI NIH HHS/United States
- N01 HC055019/HC/NHLBI NIH HHS/United States
- N01-HC-55019/HC/NHLBI NIH HHS/United States
- N01-HC-55015/HC/NHLBI NIH HHS/United States
- 1 R01 DK076770-01/DK/NIDDK NIH HHS/United States
- N01-HC-55020/HC/NHLBI NIH HHS/United States
- N01 HC055020/HC/NHLBI NIH HHS/United States
- N01-HC-55018/HC/NHLBI NIH HHS/United States
- N01 HC055016/HC/NHLBI NIH HHS/United States
- R01 DK076770/DK/NIDDK NIH HHS/United States
- N01 HC055015/HC/NHLBI NIH HHS/United States
- N01 HC055021/HC/NHLBI NIH HHS/United States
- U01 DK085689/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
