

Effect of QRS morphology on clinical event reduction with cardiac resynchronization therapy: meta-analysis of randomized controlled trials
- PMID: 22305845
- PMCID: PMC4113034
- DOI: 10.1016/j.ahj.2011.11.014
Effect of QRS morphology on clinical event reduction with cardiac resynchronization therapy: meta-analysis of randomized controlled trials
Abstract
Background: Cardiac resynchronization therapy (CRT) is effective in reducing clinical events in systolic heart failure patients with a wide QRS. Previous retrospective studies suggest only patients with QRS prolongation due to a left bundle-branch block (LBBB) benefit from CRT. Our objective was to examine this by performing a meta-analysis of all randomized controlled trials of CRT.
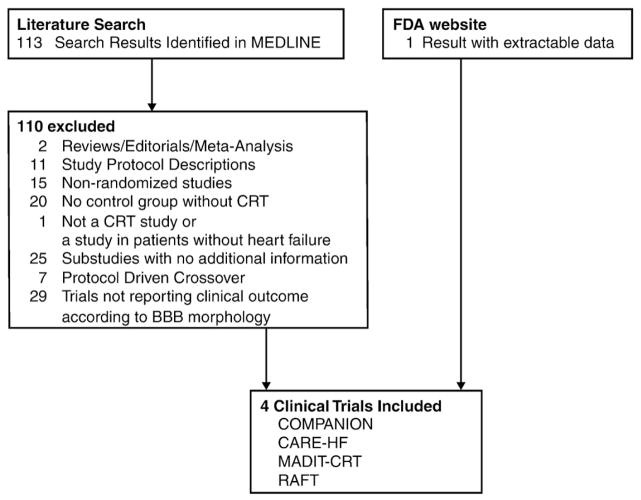
Methods: Systematic searches of MEDLINE and the Food and Drug Administration official website were conducted for randomized controlled CRT trials. Trials reporting adverse clinical events (eg, all-cause mortality, heart failure hospitalizations) according to QRS morphology were included in the meta-analysis.
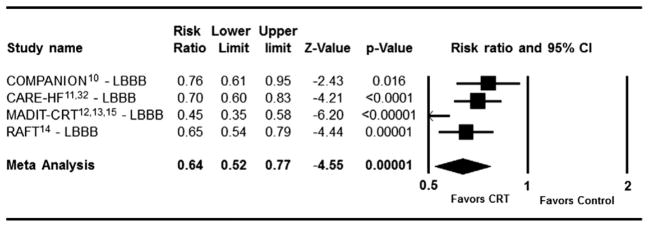
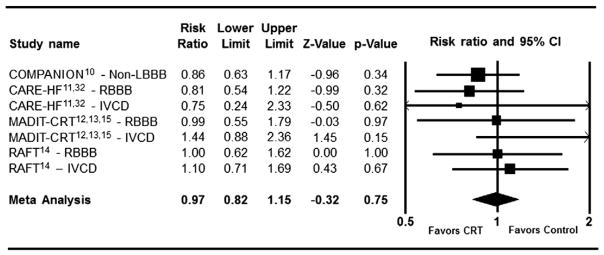
Results: Four randomized trials totaling 5,356 patients met the inclusion criteria. In patients with LBBB at baseline, there was a highly significant reduction in composite adverse clinical events with CRT (RR = 0.64 [95% CI (0.52-0.77)], P = .00001). However no such benefit was observed for patients with non-LBBB conduction abnormalities (RR = 0.97 [95% CI (0.82-1.15)], P = .75). When examined separately, there was no benefit in patients with right-bundle branch block (RR = 0.91 [95% CI (0.69-1.20)], P = .49) or non-specific intraventricular conduction delay (RR = 1.19 [95% CI (0.87-1.63)], P = .28). There was no heterogeneity among the clinical trials with regards to the lack of benefit in non-LBBB patients (I(2) = 0%). When directly compared, the difference in effect of CRT between LBBB versus non-LBBB patients was highly statistically significant (P = .0001 by heterogeneity analysis).
Conclusions: While CRT was very effective in reducing clinical events in patients with LBBB, it did not reduce such events in patients with wide QRS due to other conduction abnormalities.
Copyright © 2012 Mosby, Inc. All rights reserved.
Figures
References
-
- Rodeheffer R, Redfield M. Heart failure: diagnosis and evaluation. In: Murphy JG, Lloyd MA, editors. Mayo Clinic Cardiology. 3. Rochester (Minn): Mayo Clinic Scientific Press; 2007. pp. 1101–12.
-
- Bradley DJ, Bradley EA, Baughman KL, et al. Cardiac resynchronization and death from progressive heart failure: a meta-analysis of randomized controlled trials. JAMA. 2003;289:730–40. - PubMed
-
- McAlister FA, Ezekowitz J, Hooton N, et al. Cardiac resynchronization therapy for patients with left ventricular systolic dysfunction: a systematic review. JAMA. 2007;297:2502–14. - PubMed
-
- Executive summary: HFSA 2006 Comprehensive Heart Failure Practice Guideline. J Card Fail. 2006;12:10–38. - PubMed
-
- Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Circulation. 2008;117:e350–408. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
