

A novel automated platform for quantifying the extent of skeletal tumour involvement in prostate cancer patients using the Bone Scan Index
- PMID: 22306323
- PMCID: PMC3402084
- DOI: 10.1016/j.eururo.2012.01.037
A novel automated platform for quantifying the extent of skeletal tumour involvement in prostate cancer patients using the Bone Scan Index
Abstract
Background: There is little consensus on a standard approach to analysing bone scan images. The Bone Scan Index (BSI) is predictive of survival in patients with progressive prostate cancer (PCa), but the popularity of this metric is hampered by the tedium of the manual calculation.
Objective: Develop a fully automated method of quantifying the BSI and determining the clinical value of automated BSI measurements beyond conventional clinical and pathologic features.
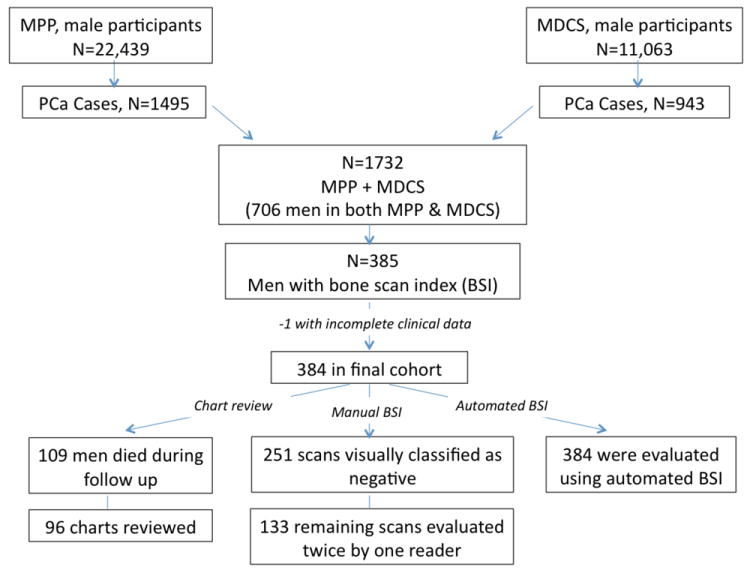
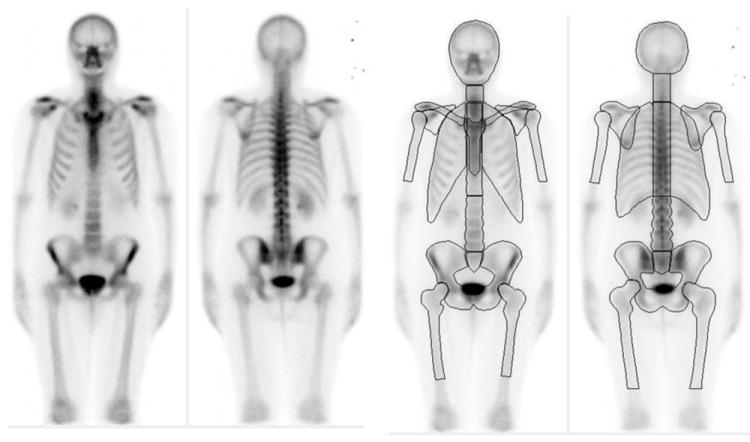
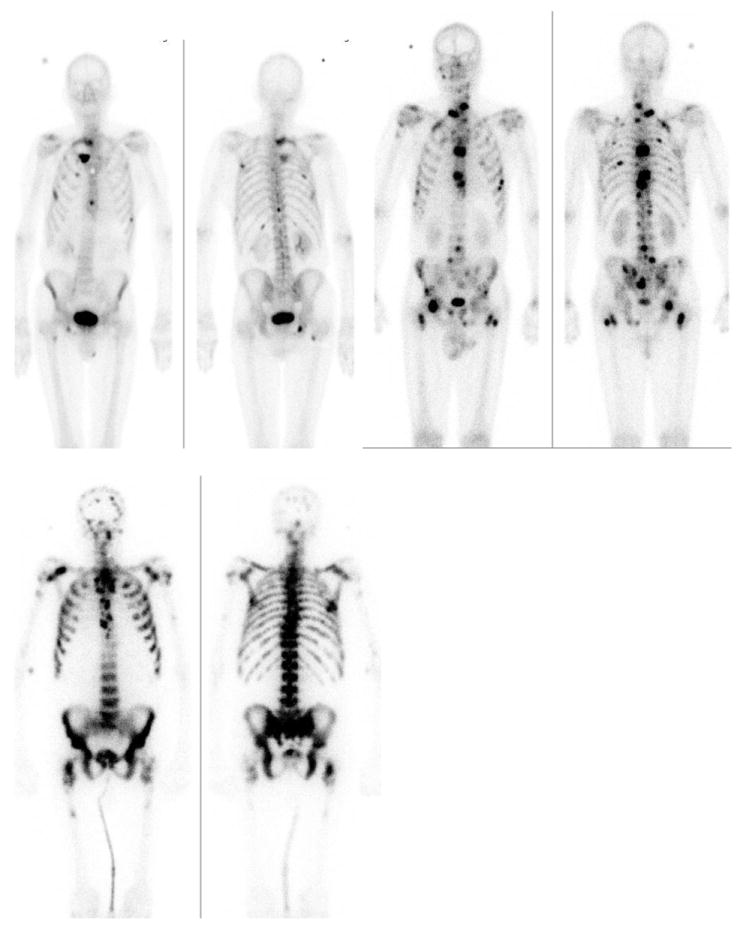
Design, setting, and participants: We conditioned a computer-assisted diagnosis system identifying metastatic lesions on a bone scan to automatically compute BSI measurements. A training group of 795 bone scans was used in the conditioning process. Independent validation of the method used bone scans obtained ≤3 mo from diagnosis of 384 PCa cases in two large population-based cohorts. An experienced analyser (blinded to case identity, prior BSI, and outcome) scored the BSI measurements twice. We measured prediction of outcome using pretreatment Gleason score, clinical stage, and prostate-specific antigen with models that also incorporated either manual or automated BSI measurements.
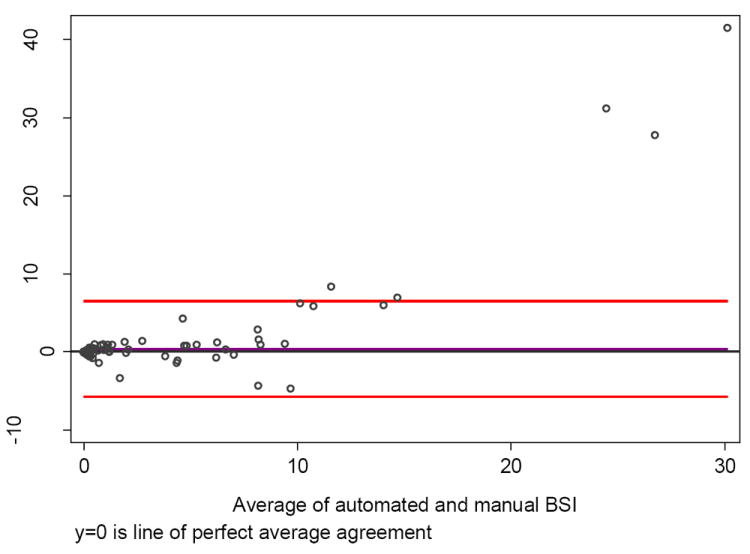
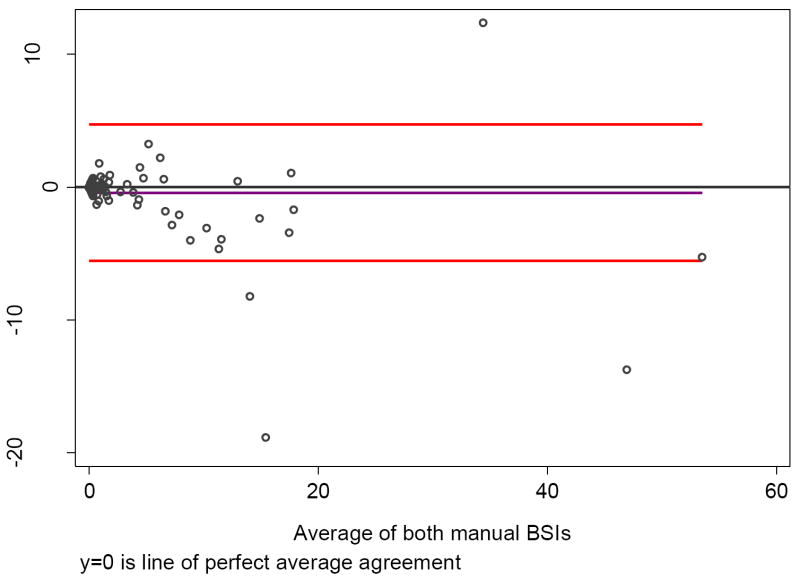
Measurements: The agreement between methods was evaluated using Pearson's correlation coefficient. Discrimination between prognostic models was assessed using the concordance index (C-index).
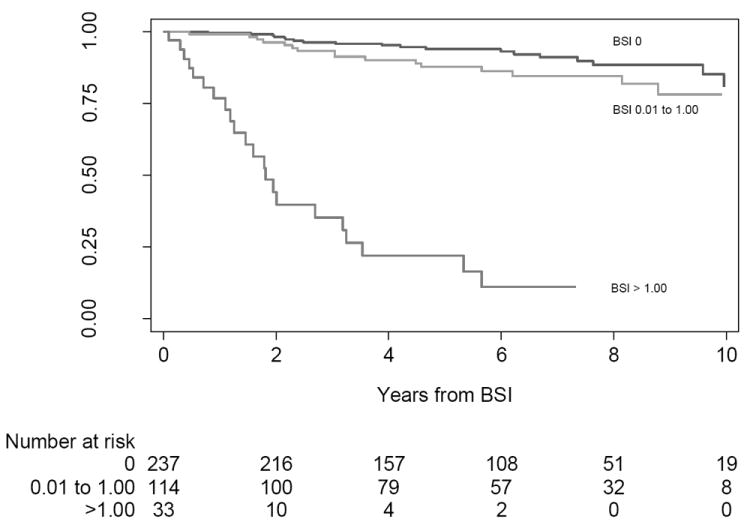
Results and limitations: Manual and automated BSI measurements were strongly correlated (ρ=0.80), correlated more closely (ρ=0.93) when excluding cases with BSI scores≥10 (1.8%), and were independently associated with PCa death (p<0.0001 for each) when added to the prediction model. Predictive accuracy of the base model (C-index: 0.768; 95% confidence interval [CI], 0.702-0.837) increased to 0.794 (95% CI, 0.727-0.860) by adding manual BSI scoring, and increased to 0.825 (95% CI, 0.754-0.881) by adding automated BSI scoring to the base model.
Conclusions: Automated BSI scoring, with its 100% reproducibility, reduces turnaround time, eliminates operator-dependent subjectivity, and provides important clinical information comparable to that of manual BSI scoring.
Copyright © 2012 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Objective evaluation of bone metastases in prostate cancer: to what end?Eur Urol. 2012 Jul;62(1):85-7. doi: 10.1016/j.eururo.2012.02.021. Epub 2012 Feb 20. Eur Urol. 2012. PMID: 22402111 No abstract available.
References
-
- Jacobs SC. Spread of prostatic cancer to bone. Urology. 1983;21:337–44. - PubMed
-
- Soloway MS, Hardeman SW, Hickey D, et al. Stratification of patients with metastatic prostate cancer based on extent of disease on initial bone scan. Cancer. 1988;61:195–202. - PubMed
-
- Cooper CR, Chay CH, Gendernalik JD, et al. Stromal factors involved in prostate carcinoma metastasis to bone. Cancer. 2003;97:739–47. - PubMed
-
- Carlin BI, Andriole GL. The natural history, skeletal complications, and management of bone metastases in patients with prostate carcinoma. Cancer. 2000;88:2989–94. - PubMed
-
- Mease RC. Radionuclide based imaging of prostate cancer. Curr Top Med Chem. 2010;10:1600–16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
