

Development and implementation of a web-enabled 3D consultation tool for breast augmentation surgery based on 3D-image reconstruction of 2D pictures
- PMID: 22306688
- PMCID: PMC3374529
- DOI: 10.2196/jmir.1903
Development and implementation of a web-enabled 3D consultation tool for breast augmentation surgery based on 3D-image reconstruction of 2D pictures
Abstract
Background: Producing a rich, personalized Web-based consultation tool for plastic surgeons and patients is challenging.
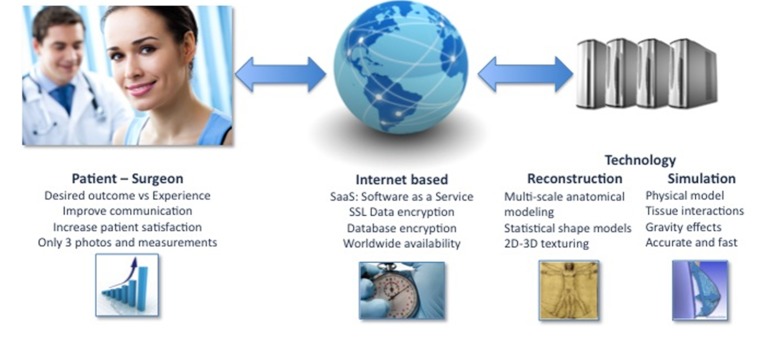
Objective: (1) To develop a computer tool that allows individual reconstruction and simulation of 3-dimensional (3D) soft tissue from ordinary digital photos of breasts, (2) to implement a Web-based, worldwide-accessible preoperative surgical planning platform for plastic surgeons, and (3) to validate this tool through a quality control analysis by comparing 3D laser scans of the patients with the 3D reconstructions with this tool from original 2-dimensional (2D) pictures of the same patients.
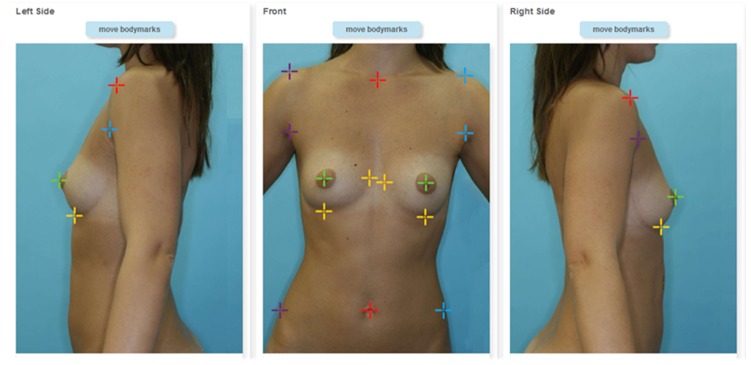
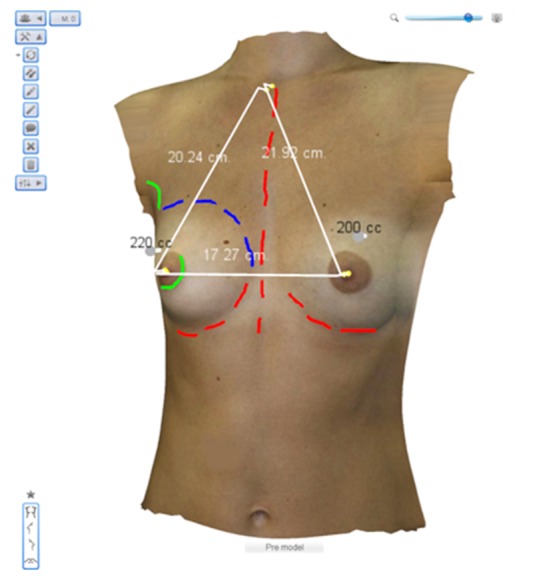
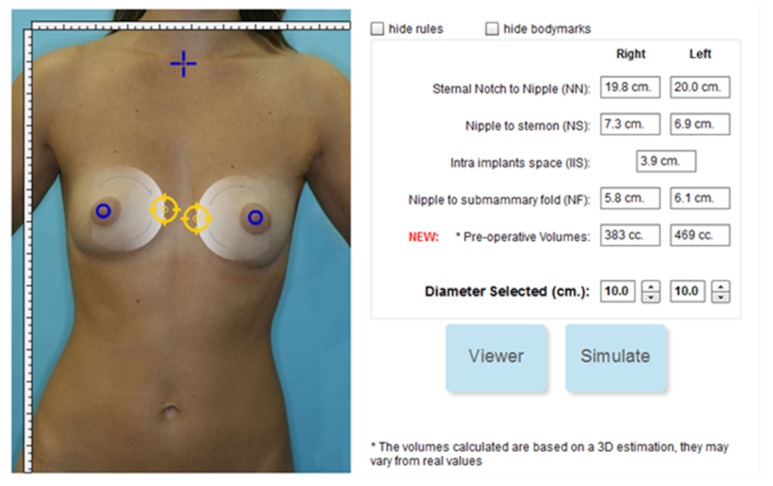
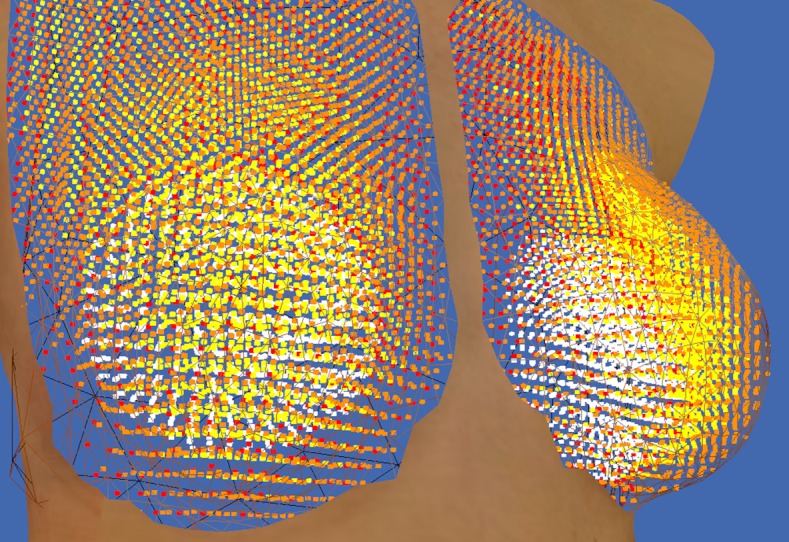
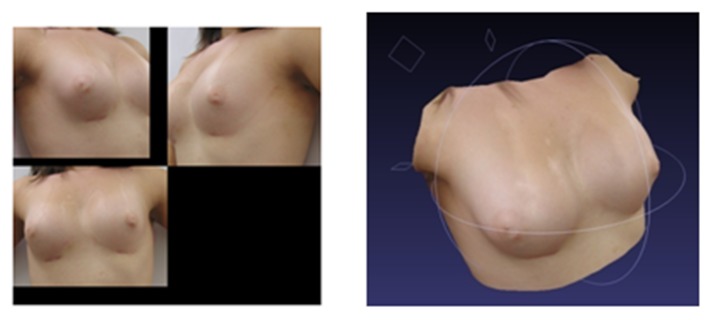
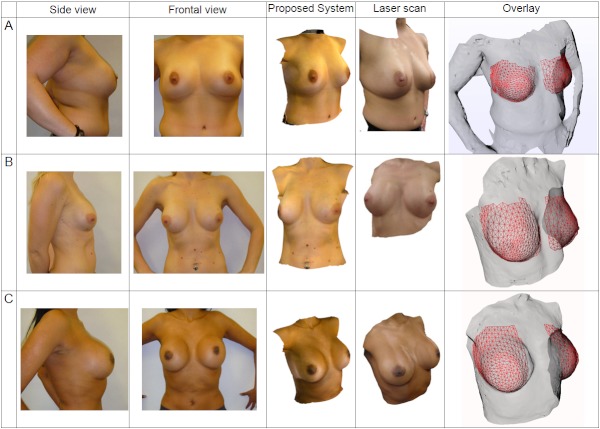
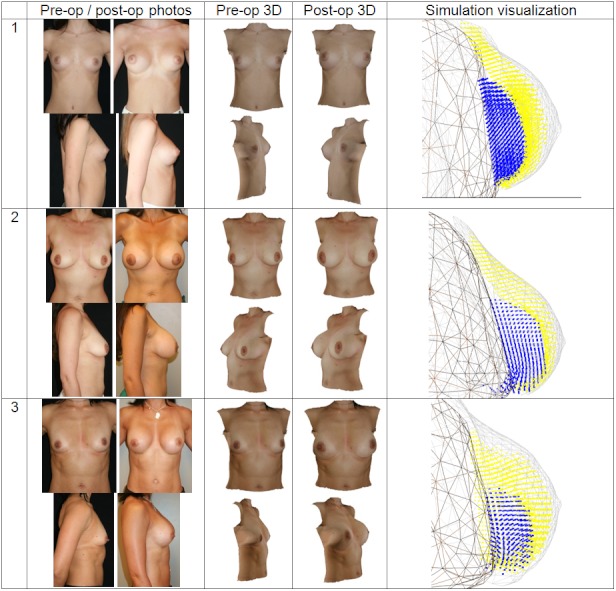
Methods: The proposed system uses well-established 2D digital photos for reconstruction into a 3D torso, which is then available to the user for interactive planning. The simulation is performed on dedicated servers, accessible via Internet. It allows the surgeon, together with the patient, to previsualize the impact of the proposed breast augmentation directly during the consultation before a surgery is decided upon. We retrospectively conduced a quality control assessment of available anonymized pre- and postoperative 2D digital photographs of patients undergoing breast augmentation procedures. The method presented above was used to reconstruct 3D pictures from 2D digital pictures. We used a laser scanner capable of generating a highly accurate surface model of the patient's anatomy to acquire ground truth data. The quality of the computed 3D reconstructions was compared with the ground truth data used to perform both qualitative and quantitative evaluations.
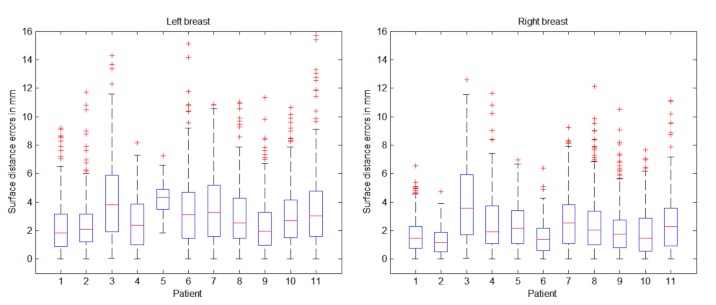
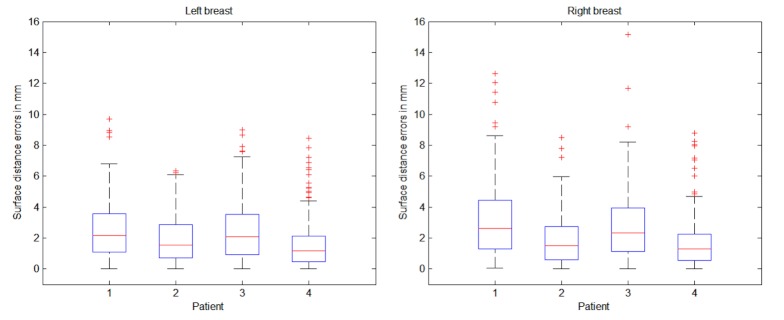
Results: We evaluated the system on 11 clinical cases for surface reconstructions and 4 clinical cases of postoperative simulations, using laser surface scan technologies showing a mean reconstruction error between 2 and 4 mm and a maximum outlier error of 16 mm. Qualitative and quantitative analyses from plastic surgeons demonstrate the potential of these new emerging technologies.
Conclusions: We tested our tool for 3D, Web-based, patient-specific consultation in the clinical scenario of breast augmentation. This example shows that the current state of development allows for creation of responsive and effective Web-based, 3D medical tools, even with highly complex and time-consuming computation, by off-loading them to a dedicated high-performance data center. The efficient combination of advanced technologies, based on analysis and understanding of human anatomy and physiology, will allow the development of further Web-based reconstruction and predictive interfaces at different scales of the human body. The consultation tool presented herein exemplifies the potential of combining advancements in the core areas of computer science and biomedical engineering with the evolving areas of Web technologies. We are confident that future developments based on a multidisciplinary approach will further pave the way toward personalized Web-enabled medicine.
Conflict of interest statement
Dr Garcia is co-owner of, and receives income from, Crisalix, S.A, which is developing products related to the research described in this paper and developed through the Swiss Agency KTI for promotion of medical technologies. The terms of this arrangement have been reviewed and approved by the University of Bern, Switzerland, in accordance with their respective conflict of interest policies.
Figures
Similar articles
-
Advancing Progressive Web Applications to Leverage Medical Imaging for Visualization of Digital Imaging and Communications in Medicine and Multiplanar Reconstruction: Software Development and Validation Study.JMIR Med Inform. 2024 Dec 9;12:e63834. doi: 10.2196/63834. JMIR Med Inform. 2024. PMID: 39652391 Free PMC article.
-
3D face reconstruction from 2D pictures: first results of a web-based computer aided system for aesthetic procedures.Ann Biomed Eng. 2013 May;41(5):952-66. doi: 10.1007/s10439-013-0744-3. Epub 2013 Jan 15. Ann Biomed Eng. 2013. PMID: 23319167
-
Customized planning of augmentation mammaplasty with silicon implants using three-dimensional optical body scans and biomechanical modeling of soft tissue outcome.Aesthetic Plast Surg. 2011 Aug;35(4):494-501. doi: 10.1007/s00266-010-9642-3. Epub 2010 Dec 24. Aesthetic Plast Surg. 2011. PMID: 21184065
-
Three-dimensional Imaging and Simulation in Breast Augmentation: What Is the Current State of the Art?Clin Plast Surg. 2015 Oct;42(4):437-50. doi: 10.1016/j.cps.2015.06.013. Epub 2015 Aug 11. Clin Plast Surg. 2015. PMID: 26408435 Review.
-
Three-dimensional imaging and three-dimensional printing for plastic preparation of medical interventions.Radiologe. 2020 Nov;60(Suppl 1):70-79. doi: 10.1007/s00117-020-00739-6. Radiologe. 2020. PMID: 32926194 Review. English.
Cited by
-
Accurate nonrigid 3D human body surface reconstruction using commodity depth sensors.Comput Animat Virtual Worlds. 2018 Sep-Oct;29(5):e1807. doi: 10.1002/cav.1807. Epub 2018 May 10. Comput Animat Virtual Worlds. 2018. PMID: 31156352 Free PMC article.
-
3D Shape-Based Body Composition Inference Model Using a Bayesian Network.IEEE J Biomed Health Inform. 2020 Jan;24(1):205-213. doi: 10.1109/JBHI.2019.2903190. Epub 2019 Mar 5. IEEE J Biomed Health Inform. 2020. PMID: 30843854 Free PMC article.
-
Use of Smartphone-Based Head-Mounted Display Devices to View a Three-Dimensional Dissection Model in a Virtual Reality Environment: Pilot Questionnaire Study.JMIR Med Educ. 2019 Jan 14;5(1):e11921. doi: 10.2196/11921. JMIR Med Educ. 2019. PMID: 31344673 Free PMC article.
-
Breast volumetric analysis for aesthetic planning in breast reconstruction: a literature review of techniques.Gland Surg. 2016 Apr;5(2):212-26. doi: 10.3978/j.issn.2227-684X.2015.10.03. Gland Surg. 2016. PMID: 27047788 Free PMC article. Review.
-
Fall Prevention Self-Assessments Via Mobile 3D Visualization Technologies: Community Dwelling Older Adults' Perceptions of Opportunities and Challenges.JMIR Hum Factors. 2017 Jun 19;4(2):e15. doi: 10.2196/humanfactors.7161. JMIR Hum Factors. 2017. PMID: 28630034 Free PMC article.
References
-
- Dwyer SJ III. A personalized view of the history of PACS in the USA. Medical Imaging 2000: PACS Design and Evaluation: Engineering and Clinical Issues; Feb 15, 2000; San Diego, CA, USA. 2000. - DOI
-
- Sicurello F, Pizzi R. TME10/380: remote transmission of radiological images by means of Intranet/Internet technology. J Med Internet Res. 1999;1(suppl 1):e117. doi: 10.2196/jmir.1. - DOI
-
- Menegaz G, Grewe L, Lozano A, Thiran JP. TME12/400: application oriented wavelet-based coding of volumetric medical data. J Med Internet Res. 1999;1(suppl 1):e119. doi: 10.2196/jmir.1. - DOI
-
- Ferrer-Roca O, Vilarchao-Cavia J, Troyano-Luque JM, Clavijo M. Virtual sonography through the Internet: volume compression issues. J Med Internet Res. 2001;3(2):E21. doi: 10.2196/jmir.3.2.e21. http://www.jmir.org/2001/2/e21/ - DOI - PMC - PubMed
-
- Coveney PV, Diaz V, Hunter P, Kohl P, Viceconti M. The virtual physiological human. Interface Focus. 2011;1:281–5. doi: 10.1098/rsfs.2011.0020. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
