

A review of cancer in U.S. Hispanic populations
- PMID: 22307564
- PMCID: PMC5815320
- DOI: 10.1158/1940-6207.CAPR-11-0447
A review of cancer in U.S. Hispanic populations
Abstract
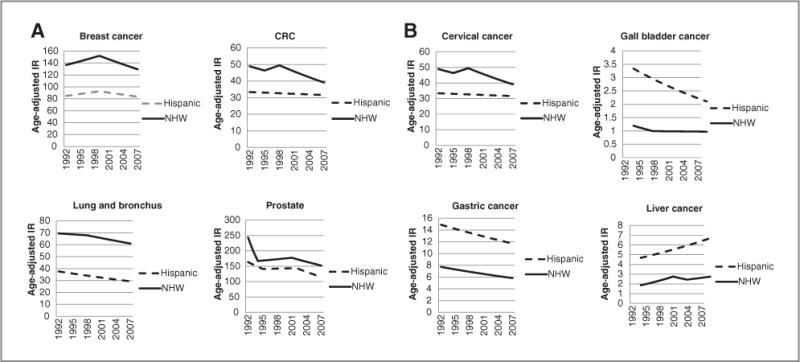
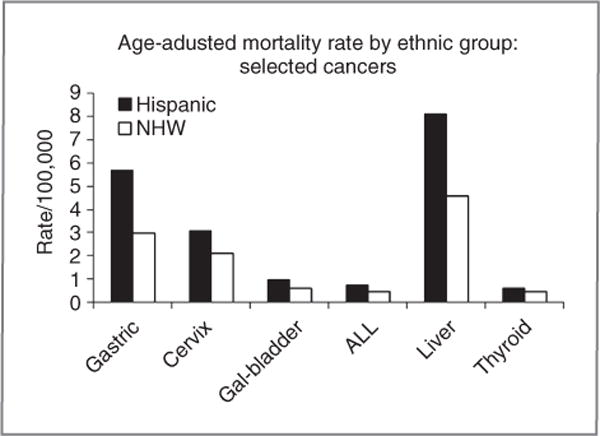
There are compelling reasons to conduct studies of cancer in Hispanics, the fastest growing major demographic group in the United States (from 15% to 30% of the U.S. population by 2050). The genetically admixed Hispanic population coupled with secular trends in environmental exposures and lifestyle/behavioral practices that are associated with immigration and acculturation offer opportunities for elucidating the effects of genetics, environment, and lifestyle on cancer risk and identifying novel risk factors. For example, traditional breast cancer risk factors explain less of the breast cancer risk in Hispanics than in non-Hispanic whites (NHW), and there is a substantially greater proportion of never-smokers with lung cancer in Hispanics than in NHW. Hispanics have higher incidence rates for cancers of the cervix, stomach, liver, and gall bladder than NHW. With respect to these cancers, there are intriguing patterns that warrant study (e.g., depending on country of origin, the five-fold difference in gastric cancer rates for Hispanic men but not Hispanic women). Also, despite a substantially higher incidence rate and increasing secular trend for liver cancer in Hispanics, there have been no studies of Hispanics reported to date. We review the literature and discuss study design options and features that should be considered in future studies.
©2011 AACR.
Conflict of interest statement
No potential conflicts of interests were disclosed.
Figures
References
-
- Vargas Bustamante A, Chen J, Rodriguez HP, Rizzo JA, Ortega AN. Use of preventive care services among Latino subgroups. Am J Prev Med. 2010;38:610–9. - PubMed
-
- Zambrana RE, Breen N, Fox SA, Gutierrez-Mohamed ML. Use of cancer screening practices by Hispanic women: analyses by subgroup. Prev Med. 1999;29:466–77. - PubMed
-
- Gorin SS, Heck JE. Cancer screening among Latino subgroups in the United States. Prev Med. 2005;40:515–26. - PubMed
-
- Shah M, Zhu K, Potter J. Hispanic acculturation and utilization of colorectal cancer screening in the United States. Cancer Detect Prev. 2006;30:306–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
