

Assessing left ventricular systolic dysfunction after myocardial infarction: are ejection fraction and dP/dt(max) complementary or redundant?
- PMID: 22307667
- PMCID: PMC3330783
- DOI: 10.1152/ajpheart.01211.2011
Assessing left ventricular systolic dysfunction after myocardial infarction: are ejection fraction and dP/dt(max) complementary or redundant?
Abstract
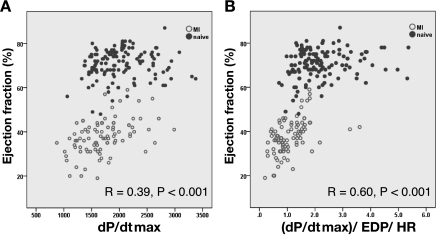
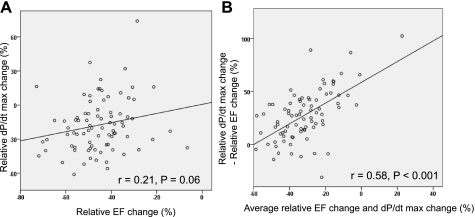
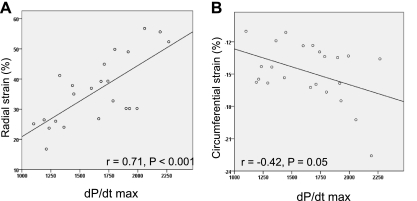
Among the various cardiac contractility parameters, left ventricular (LV) ejection fraction (EF) and maximum dP/dt (dP/dt(max)) are the simplest and most used. However, these parameters are often reported together, and it is not clear if they are complementary or redundant. We sought to compare the discriminative value of EF and dP/dt(max) in assessing systolic dysfunction after myocardial infarction (MI) in swine. A total of 220 measurements were obtained. All measurements included LV volumes and EF analysis by left ventriculography, invasive ventricular pressure tracings, and echocardiography. Baseline measurements were performed in 132 pigs, and 88 measurements were obtained at different time points after MI creation. Receiver operator characteristic (ROC) curves to distinguish the presence or absence of an MI revealed a good predictive value for EF [area under the curve (AUC): 0.998] but not by dP/dt(max) (AUC: 0.69, P < 0.001 vs. EF). Dividing dP/dt(max) by LV end-diastolic pressure and heart rate (HR) significantly increased the AUC to 0.87 (P < 0.001 vs. dP/dt(max) and P < 0.001 vs. EF). In naïve pigs, the coefficient of variation of dP/dt(max) was twice than that of EF (22.5% vs. 9.5%, respectively). Furthermore, in n = 19 pigs, dP/dt(max) increased after MI. However, echocardiographic strain analysis of 23 pigs with EF ranging only from 36% to 40% after MI revealed significant correlations between dP/dt(max) and strain parameters in the noninfarcted area (circumferential strain: r = 0.42, P = 0.05; radial strain: r = 0.71, P < 0.001). In conclusion, EF is a more accurate measure of systolic dysfunction than dP/dt(max) in a swine model of MI. Despite the variability of dP/dt(max) both in naïve pigs and after MI, it may sensitively reflect the small changes of myocardial contractility.
Figures



References
-
- Aghajani E, Muller S, Kjorstad KE, Korvald C, Nordhaug D, Revhaugand A, Myrmel T. The pressure-volume loop revisited: Is the search for a cardiac contractility index a futile cycle? Shock 25: 370–376, 2006 - PubMed
-
- Belghitia H, Brette S, Lafitte S, Reant P, Picard F, Serri K, Lafitte M, Courregelongue M, Dos Santos P, Douard H, Roudaut R, DeMaria A. Automated function imaging: a new operator-independent strain method for assessing left ventricular function. Arch Cardiovasc Dis 101: 163–169, 2008 - PubMed
-
- Bolognesi R, Tsialtas D, Zeppellini R, Barilli AL, Cucchini F, Manca C. Early and subtle abnormalities of left ventricular function in clinically stable coronary artery disease patients with normal ejection fraction. J Card Fail 10: 304–309, 2004 - PubMed
-
- Cohn JN, Johnson GR, Shabetai R, Loeb H, Tristani F, Rector T, Smith R, Fletcher R. Ejection fraction, peak exercise oxygen consumption, cardiothoracic ratio, ventricular arrhythmias, and plasma norepinephrine as determinants of prognosis in heart failure. The V-HeFT VA Cooperative Studies Group Circulation 87: VI5–V16, 1993 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical