

Silent intralesional microhemorrhage as a risk factor for brain arteriovenous malformation rupture
- PMID: 22308253
- PMCID: PMC3335931
- DOI: 10.1161/STROKEAHA.111.647263
Silent intralesional microhemorrhage as a risk factor for brain arteriovenous malformation rupture
Abstract
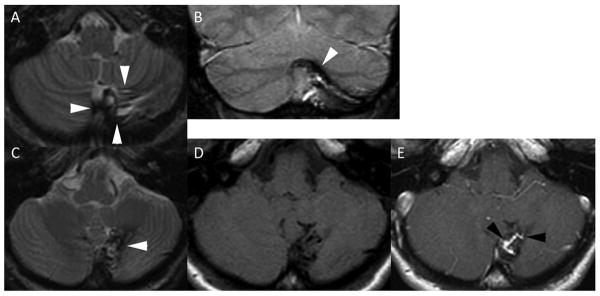
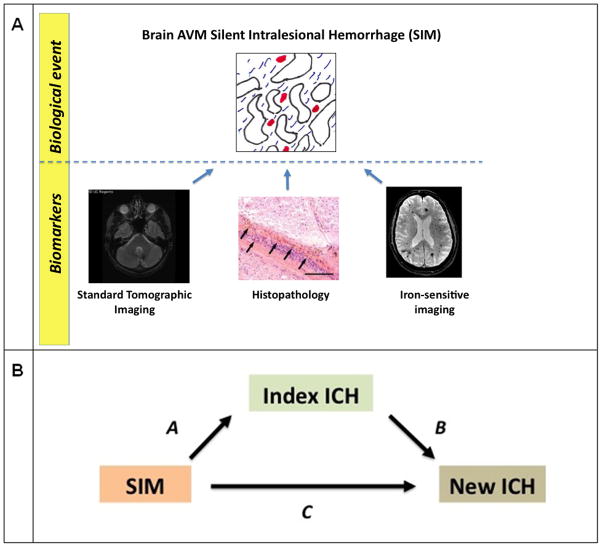
Background and purpose: We investigated whether brain arteriovenous malformation silent intralesional microhemorrhage, that is, asymptomatic bleeding in the nidal compartment, might serve as a marker for increased risk of symptomatic intracranial hemorrhage (ICH). We evaluated 2 markers to assess the occurrence of silent intralesional microhemorrhage: neuroradiological assessment of evidence of old hemorrhage-imaging evidence of bleeding before the outcome events-and hemosiderin positivity in hematoxylin and eosin-stained paraffin block sections.
Methods: We identified cases from our brain arteriovenous malformation database with recorded neuroradiological data or available surgical paraffin blocks. Using 2 end points, index ICH or new ICH after diagnosis (censored at treatment, loss to follow-up, or death), we performed logistic or Cox regression to assess evidence of old hemorrhage and hemosiderin positivity adjusting for age, sex, deep-only venous drainage, maximal brain arteriovenous malformation size, deep location, and associated arterial aneurysms.
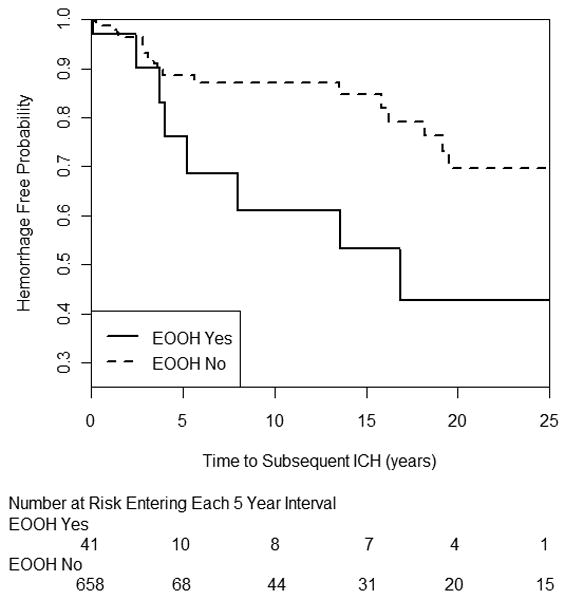
Results: Evidence of old hemorrhage was present in 6.5% (n=975) of patients and highly predictive of index ICH (P<0.001; OR, 3.97; 95% CI, 2.1-7.5) adjusting for other risk factors. In a multivariable model (n=643), evidence of old hemorrhage was an independent predictor of new ICH (hazard ratio, 3.53; 95% CI, 1.35-9.23; P=0.010). Hemosiderin positivity was found in 36.2% (29.6% in unruptured; 47.8% in ruptured; P=0.04) and associated with index ICH in univariate (OR, 2.18; 95% CI, 1.03-4.61; P=0.042; n=127) and multivariable models (OR, 3.64; 95% CI, 1.11-12.00; P=0.034; n=79).
Conclusions: The prevalence of silent intralesional microhemorrhage is high and there is evidence for an association with both index and subsequent ICH. Further development of means to detect silent intralesional microhemorrhage during brain arteriovenous malformation evaluation may present an opportunity to improve risk stratification, especially for unruptured brain arteriovenous malformations.
Figures
References
-
- Kim H, Sidney S, McCulloch CE, Poon KY, Singh V, Johnston SC, et al. Racial/ethnic differences in longitudinal risk of intracranial hemorrhage in brain arteriovenous malformation patients. Stroke. 2007;38:2430–2437. - PubMed
-
- Stapf C, Mast H, Sciacca RR, Choi JH, Khaw AV, Connolly ES, et al. Predictors of hemorrhage in patients with untreated brain arteriovenous malformation. Neurology. 2006;66:1350–1355. - PubMed
-
- Stein BM, Wolpert SM. Arteriovenous malformations of the brain. I: Current concepts and treatment. Arch Neurol. 1980;37:1–5. - PubMed
-
- Prayer L, Wimberger D, Stiglbauer R, Kramer J, Richling B, Bavinzski G, et al. Haemorrhage in intracerebral arteriovenous malformations: detection with MRI and comparison with clinical history. Neuroradiology. 1993;35:424–427. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
