

Neurocognitive and motor deficits in HIV-infected Ugandan children with high CD4 cell counts
- PMID: 22308272
- PMCID: PMC3297647
- DOI: 10.1093/cid/cir1037
Neurocognitive and motor deficits in HIV-infected Ugandan children with high CD4 cell counts
Abstract
Background: Human immunodeficiency virus (HIV) infection causes neurocognitive or motor function deficits in children with advanced disease, but it is unclear whether children with CD4 cell measures above the World Health Organization (WHO) thresholds for antiretroviral therapy (ART) initiation suffer significant impairment.
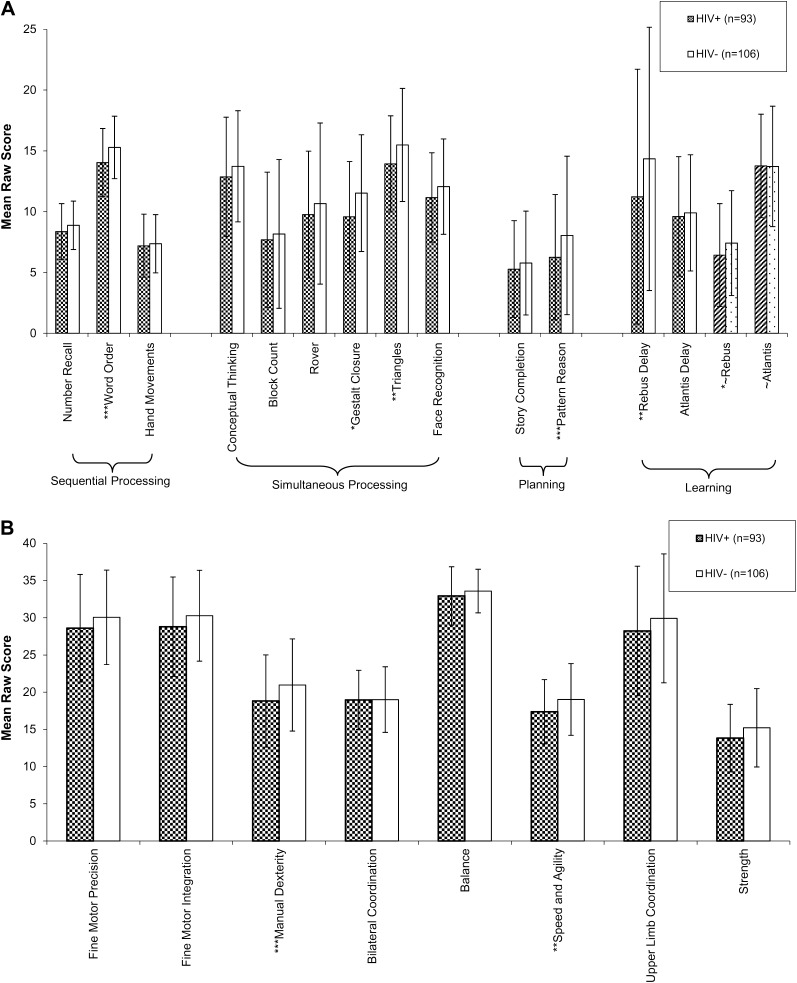
Methods: The neurocognitive and motor functions of HIV-infected ART-naive Ugandan children aged 6-12 years with CD4 cell counts of >350 cells/μL and CD4 cell percentage of >15% were compared with those of HIV-uninfected children, using the Test of Variables of Attention (TOVA), the Kaufman Assessment Battery for Children, second edition (KABC-2), and the Bruininks-Oseretsky Test of Motor Proficiency, second edition (BOT-2).
Results: Ninety-three HIV-infected children (median CD4 cell count, 655 cells/μL; plasma HIV RNA level, 4.7 log(10) copies/mL) were compared to 106 HIV-uninfected children. HIV-infected children performed worse on TOVA visual reaction times (multivariate analysis of covariance; P = .006); KABC-2 sequential processing (P = .005), simultaneous processing (P = .039), planning/reasoning (P = .023), and global performance (P = .024); and BOT-2 total motor proficiency (P = .003). High plasma HIV RNA level was associated with worse performance in 10 cognitive measures and 3 motor measures. In analysis of only WHO clinical stage 1 or 2 HIV-infected children (n = 68), significant differences between the HIV-infected and HIV-uninfected groups (P < .05) remained for KABC-2 sequential processing, KABC-2 planning/reasoning, and BOT-2 motor proficiency.
Conclusions: Significant motor and cognitive deficits were found in HIV-infected ART-naive Ugandan children with CD4 cell counts of ∼350 cells/μL and percentages of >15%. Study of whether early initiation of ART could prevent or reverse such deficits is needed.
Figures
Comment in
-
Yet another reason to treat HIV infection.Clin Infect Dis. 2012 Apr;54(7):1010-2. doi: 10.1093/cid/cir1041. Epub 2012 Feb 4. Clin Infect Dis. 2012. PMID: 22308271 No abstract available.
References
-
- Nozyce M, Hittelman J, Muenz L, Durako SJ, Fischer ML, Willoughby A. Effect of perinatally acquired human immunodeficiency virus infection on neurodevelopment in children during the first two years of life. Pediatrics. 1994;94:883–91. - PubMed
-
- Diamond GW, Kaufman J, Belman AL, Cohen L, Cohen HJ, Rubinstein A. Characterization of cognitive functioning in a subgroup of children with congenital HIV infection. Arch Clin Neuropsychol. 1987;2:245–56. - PubMed
-
- Belman AL, Diamond G, Dickson D, et al. Pediatric acquired immunodeficiency syndrome: neurologic syndromes. Am J Dis Child. 1988;142:29–35. - PubMed
-
- Cooper ER, Hanson C, Diaz C, et al. Encephalopathy and progression of human immunodeficiency virus disease in a cohort of children with perinatally acquired human immunodeficiency virus infection. Women and Infants Transmission Study Group. J Pediatr. 1998;132:808–12. - PubMed
-
- Brouwers P, Tudor-Williams G, DeCarli C, et al. Relation between stage of disease and neurobehavioral measures in children with symptomatic HIV disease. AIDS. 1995;9:713–20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
