

Hypertension with or without adrenal hyperplasia due to different inherited mutations in the potassium channel KCNJ5
- PMID: 22308486
- PMCID: PMC3289329
- DOI: 10.1073/pnas.1121407109
Hypertension with or without adrenal hyperplasia due to different inherited mutations in the potassium channel KCNJ5
Abstract
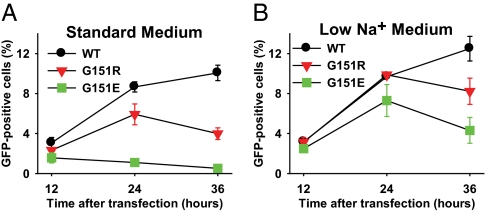
We recently implicated two recurrent somatic mutations in an adrenal potassium channel, KCNJ5, as a cause of aldosterone-producing adrenal adenomas (APAs) and one inherited KCNJ5 mutation in a Mendelian form of early severe hypertension with massive adrenal hyperplasia. The mutations identified all altered the channel selectivity filter, producing increased Na(+) conductance and membrane depolarization, the signal for aldosterone production and proliferation of adrenal glomerulosa cells. We report herein members of four kindreds with early onset primary aldosteronism of unknown cause. Sequencing of KCNJ5 revealed that affected members of two kindreds had KCNJ5(G151R) mutations, identical to one of the prevalent recurrent mutations in APAs. These individuals had severe progressive aldosteronism and hyperplasia requiring bilateral adrenalectomy in childhood for blood pressure control. Affected members of the other two kindreds had KCNJ5(G151E) mutations, which are not seen in APAs. These subjects had easily controlled hypertension and no evidence of hyperplasia. Surprisingly, electrophysiology of channels expressed in 293T cells demonstrated that KCNJ5(G151E) was the more extreme mutation, producing a much larger Na(+) conductance than KCNJ5(G151R), resulting in rapid Na(+)-dependent cell lethality. We infer that this increased lethality limits adrenocortical cell mass and the severity of aldosteronism in vivo, accounting for the milder phenotype among these patients. These findings demonstrate striking variations in phenotypes and clinical outcome resulting from different mutations of the same amino acid in KCNJ5 and have implications for the diagnosis and pathogenesis of primary aldosteronism with and without adrenal hyperplasia.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Kearney PM, et al. Global burden of hypertension: Analysis of worldwide data. Lancet. 2005;365:217–223. - PubMed
-
- Chobanian AV, et al. National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 report. JAMA. 2003;289:2560–2572. - PubMed
-
- WHO . Global Health Risks - Mortality and Burden of Disease Attributable to Selected Major Risks. Geneva: WHO; 2009.
-
- Yoon SS, Ostchega Y, Louis T. Recent trends in the prevalence of high blood pressure and its treatment and control, 1999-2008. NCHS Data Brief. 2010;(48):1–8. - PubMed
-
- Lifton RP, Gharavi AG, Geller DS. Molecular mechanisms of human hypertension. Cell. 2001;104:545–556. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
