

Practice Guideline
doi: 10.6004/jnccn.2012.0022.
Lung cancer screening
Affiliations
- PMID: 22308518
- PMCID: PMC6467530
- DOI: 10.6004/jnccn.2012.0022
Item in Clipboard
Practice Guideline
Lung cancer screening
J Natl Compr Canc Netw.
2012 Feb.
No abstract available
Conflict of interest statement
The NCCN guidelines staff have no conflicts to disclose.
Figures
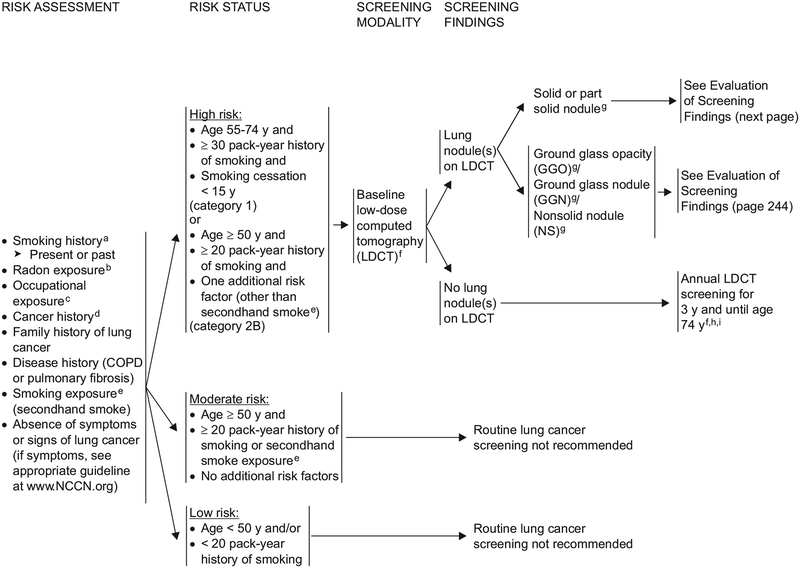
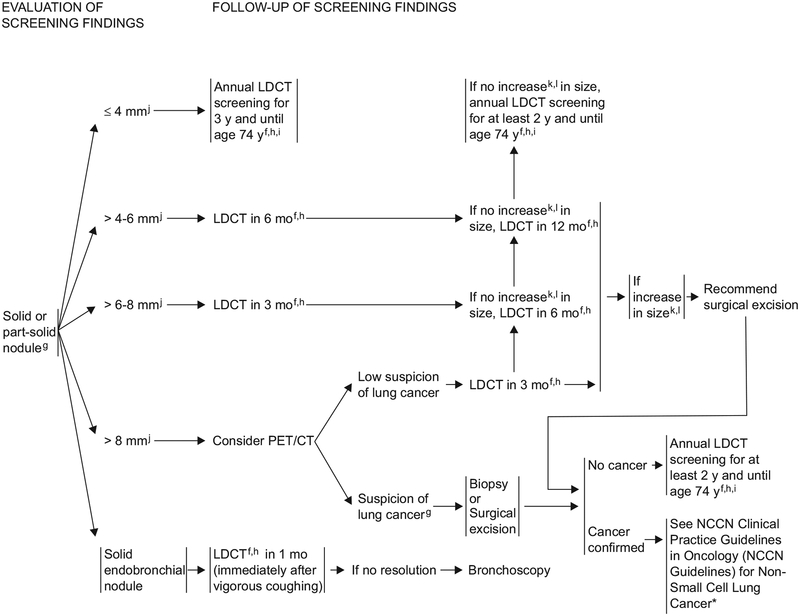
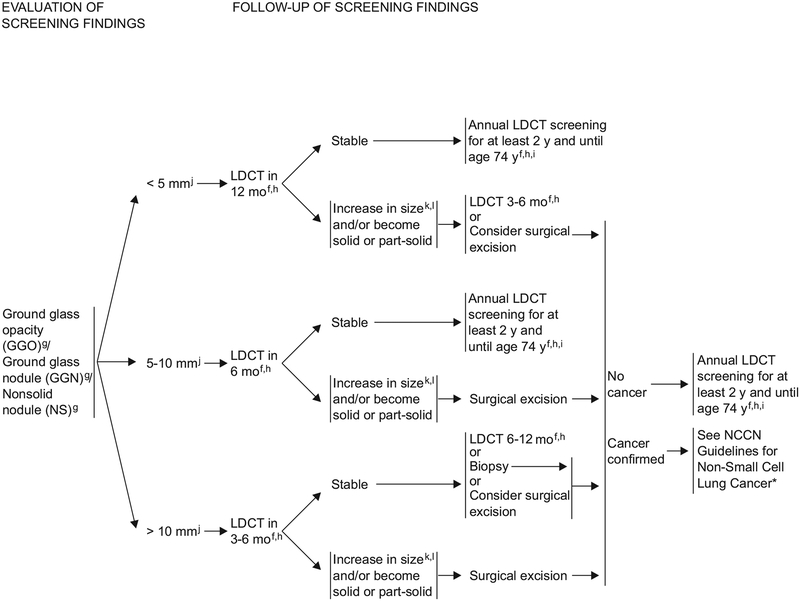
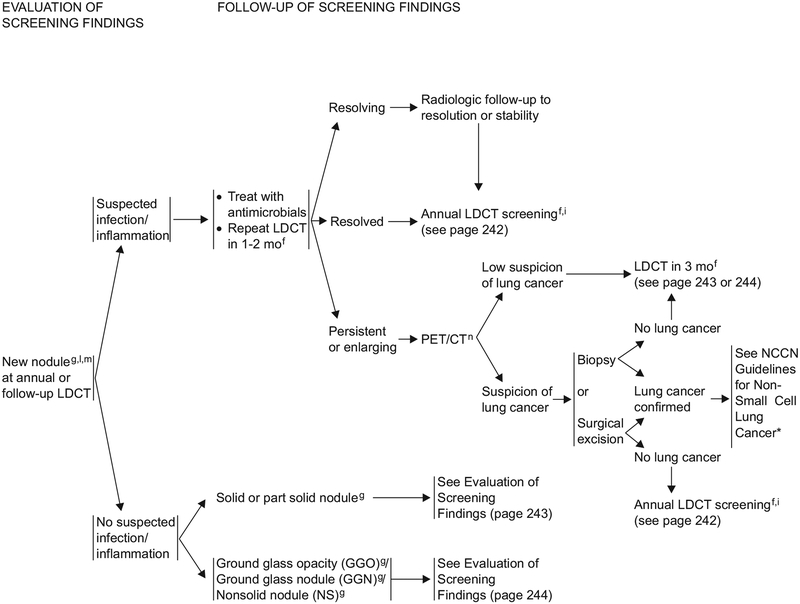
aSmokers should always be encouraged to quit smoking (http://www.smokefree.gov/ ). bDocumented high radon exposure. cAgents that are identified specifically as carcinogens targeting the lungs: silica, cadmium, asbestos, arsenic, beryllium, chromium, diesel fumes, and nickel. dThere is increased risk of developing new primary lung cancer among survivors of lung cancer, lymphomas, cancers of the head and neck, or smoking-related cancers. eIndividuals exposed to secondhand smoke have a highly variable exposure to the carcinogens, with varying evidence for increased risk after this variable exposure. Therefore, secondhand smoke is not independently considered a risk factor for lung cancer screening. fAll screening and follow-up CT scans should be performed at low dose (100–120 kVp and 40–60 mAs or less), unless evaluating mediastinal abnormalities or lymph nodes, for which standard-dose CT with IV contrast might be appropriate. gWithout benign pattern of calcification, fat in nodule as in hamartoma, or features suggesting inflammatory etiology. When multiple nodules are present and occult infection or inflammation is a possibility, an added option is a course of a broad-spectrum antibiotic with anaerobic coverage, followed by low-dose CT 1–2 mo later. hIf new nodule at annual or follow-up LDCT, see page 245. New nodule is defined as ≥ 3 mm in mean diameter iThere is uncertainty about the appropriate duration of screening and the age at which screening is no longer appropriate. jMean diameter is the mean of the longest diameter of the nodule and its perpendicular diameter when compared with the baseline scan. kFor nodules ≤ 15 mm: increase in mean diameter ≥ 2 mm in any nodule or in the solid portion of a part solid nodule compared with baseline scan. For nodules ≥ 15 mm: increase in mean diameter of ≥ 15% compared with baseline scan. lRapid increase in size should raise suspicion of inflammatory etiology or malignancy other than NSCLC. mNew nodule is defined as ≥ 3 mm in mean diameter. nPET-CT for lesions ≥ 8 mm. *To view the most recent version of these guidelines, visit the NCCN Web site at www.NCCN.org .
aSmokers should always be encouraged to quit smoking (http://www.smokefree.gov/ ). bDocumented high radon exposure. cAgents that are identified specifically as carcinogens targeting the lungs: silica, cadmium, asbestos, arsenic, beryllium, chromium, diesel fumes, and nickel. dThere is increased risk of developing new primary lung cancer among survivors of lung cancer, lymphomas, cancers of the head and neck, or smoking-related cancers. eIndividuals exposed to secondhand smoke have a highly variable exposure to the carcinogens, with varying evidence for increased risk after this variable exposure. Therefore, secondhand smoke is not independently considered a risk factor for lung cancer screening. fAll screening and follow-up CT scans should be performed at low dose (100–120 kVp and 40–60 mAs or less), unless evaluating mediastinal abnormalities or lymph nodes, for which standard-dose CT with IV contrast might be appropriate. gWithout benign pattern of calcification, fat in nodule as in hamartoma, or features suggesting inflammatory etiology. When multiple nodules are present and occult infection or inflammation is a possibility, an added option is a course of a broad-spectrum antibiotic with anaerobic coverage, followed by low-dose CT 1–2 mo later. hIf new nodule at annual or follow-up LDCT, see page 245. New nodule is defined as ≥ 3 mm in mean diameter iThere is uncertainty about the appropriate duration of screening and the age at which screening is no longer appropriate. jMean diameter is the mean of the longest diameter of the nodule and its perpendicular diameter when compared with the baseline scan. kFor nodules ≤ 15 mm: increase in mean diameter ≥ 2 mm in any nodule or in the solid portion of a part solid nodule compared with baseline scan. For nodules ≥ 15 mm: increase in mean diameter of ≥ 15% compared with baseline scan. lRapid increase in size should raise suspicion of inflammatory etiology or malignancy other than NSCLC. mNew nodule is defined as ≥ 3 mm in mean diameter. nPET-CT for lesions ≥ 8 mm. *To view the most recent version of these guidelines, visit the NCCN Web site at www.NCCN.org .
aSmokers should always be encouraged to quit smoking (http://www.smokefree.gov/ ). bDocumented high radon exposure. cAgents that are identified specifically as carcinogens targeting the lungs: silica, cadmium, asbestos, arsenic, beryllium, chromium, diesel fumes, and nickel. dThere is increased risk of developing new primary lung cancer among survivors of lung cancer, lymphomas, cancers of the head and neck, or smoking-related cancers. eIndividuals exposed to secondhand smoke have a highly variable exposure to the carcinogens, with varying evidence for increased risk after this variable exposure. Therefore, secondhand smoke is not independently considered a risk factor for lung cancer screening. fAll screening and follow-up CT scans should be performed at low dose (100–120 kVp and 40–60 mAs or less), unless evaluating mediastinal abnormalities or lymph nodes, for which standard-dose CT with IV contrast might be appropriate. gWithout benign pattern of calcification, fat in nodule as in hamartoma, or features suggesting inflammatory etiology. When multiple nodules are present and occult infection or inflammation is a possibility, an added option is a course of a broad-spectrum antibiotic with anaerobic coverage, followed by low-dose CT 1–2 mo later. hIf new nodule at annual or follow-up LDCT, see page 245. New nodule is defined as ≥ 3 mm in mean diameter iThere is uncertainty about the appropriate duration of screening and the age at which screening is no longer appropriate. jMean diameter is the mean of the longest diameter of the nodule and its perpendicular diameter when compared with the baseline scan. kFor nodules ≤ 15 mm: increase in mean diameter ≥ 2 mm in any nodule or in the solid portion of a part solid nodule compared with baseline scan. For nodules ≥ 15 mm: increase in mean diameter of ≥ 15% compared with baseline scan. lRapid increase in size should raise suspicion of inflammatory etiology or malignancy other than NSCLC. mNew nodule is defined as ≥ 3 mm in mean diameter. nPET-CT for lesions ≥ 8 mm. *To view the most recent version of these guidelines, visit the NCCN Web site at www.NCCN.org .
aSmokers should always be encouraged to quit smoking (http://www.smokefree.gov/ ). bDocumented high radon exposure. cAgents that are identified specifically as carcinogens targeting the lungs: silica, cadmium, asbestos, arsenic, beryllium, chromium, diesel fumes, and nickel. dThere is increased risk of developing new primary lung cancer among survivors of lung cancer, lymphomas, cancers of the head and neck, or smoking-related cancers. eIndividuals exposed to secondhand smoke have a highly variable exposure to the carcinogens, with varying evidence for increased risk after this variable exposure. Therefore, secondhand smoke is not independently considered a risk factor for lung cancer screening. fAll screening and follow-up CT scans should be performed at low dose (100–120 kVp and 40–60 mAs or less), unless evaluating mediastinal abnormalities or lymph nodes, for which standard-dose CT with IV contrast might be appropriate. gWithout benign pattern of calcification, fat in nodule as in hamartoma, or features suggesting inflammatory etiology. When multiple nodules are present and occult infection or inflammation is a possibility, an added option is a course of a broad-spectrum antibiotic with anaerobic coverage, followed by low-dose CT 1–2 mo later. hIf new nodule at annual or follow-up LDCT, see page 245. New nodule is defined as ≥ 3 mm in mean diameter iThere is uncertainty about the appropriate duration of screening and the age at which screening is no longer appropriate. jMean diameter is the mean of the longest diameter of the nodule and its perpendicular diameter when compared with the baseline scan. kFor nodules ≤ 15 mm: increase in mean diameter ≥ 2 mm in any nodule or in the solid portion of a part solid nodule compared with baseline scan. For nodules ≥ 15 mm: increase in mean diameter of ≥ 15% compared with baseline scan. lRapid increase in size should raise suspicion of inflammatory etiology or malignancy other than NSCLC. mNew nodule is defined as ≥ 3 mm in mean diameter. nPET-CT for lesions ≥ 8 mm. *To view the most recent version of these guidelines, visit the NCCN Web site at www.NCCN.org .
References
-
- U.S. Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004.
-
- Thun MJ, Henley SJ, Burns D, et al. Lung cancer death rates in lifelong nonsmokers. J Natl Cancer Inst 2006;98:691–699. - PubMed
-
- Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011;61:69–90. - PubMed
-
- Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin 2011;61:212–236. - PubMed
-
- Goldstraw P, Crowley J, Chansky K, et al. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol 2007;2:706–714. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
