

"GOLD or lower limit of normal definition? A comparison with expert-based diagnosis of chronic obstructive pulmonary disease in a prospective cohort-study"
- PMID: 22309369
- PMCID: PMC3299632
- DOI: 10.1186/1465-9921-13-13
"GOLD or lower limit of normal definition? A comparison with expert-based diagnosis of chronic obstructive pulmonary disease in a prospective cohort-study"
Abstract
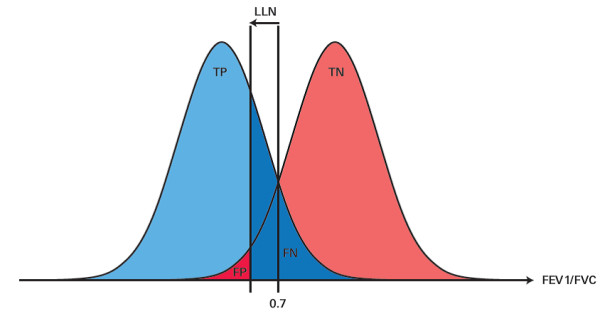
Background: The Global initiative for chronic Obstructive Lung Disease (GOLD) defines COPD as a fixed post-bronchodilator ratio of forced expiratory volume in 1 second and forced vital capacity (FEV1/FVC) below 0.7. Age-dependent cut-off values below the lower fifth percentile (LLN) of this ratio derived from the general population have been proposed as an alternative. We wanted to assess the diagnostic accuracy and prognostic capability of the GOLD and LLN definition when compared to an expert-based diagnosis.
Methods: In a prospective cohort study, 405 patients aged ≥ 65 years with a general practitioner's diagnosis of COPD were recruited and followed up for 4.5 (median; quartiles 3.9; 5.1) years. Prevalence rates of COPD according to GOLD and three LLN definitions and diagnostic performance measurements were calculated. The reference standard was the diagnosis of COPD of an expert panel that used all available diagnostic information, including spirometry and bodyplethysmography.
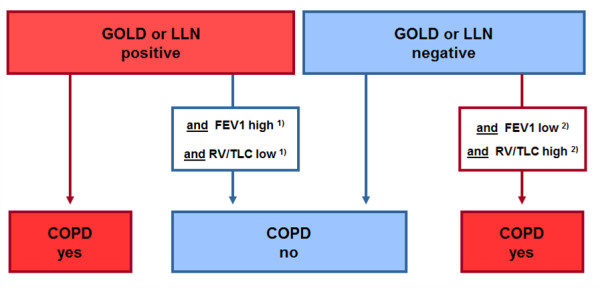
Results: Compared to the expert panel diagnosis, 'GOLD-COPD' misclassified 69 (28%) patients, and the three LLNs misclassified 114 (46%), 96 (39%), and 98 (40%) patients, respectively. The GOLD classification led to more false positives, the LLNs to more false negative diagnoses. The main predictors beyond the FEV1/FVC ratio for an expert diagnosis of COPD were the FEV1 % predicted, and the residual volume/total lung capacity ratio (RV/TLC). Adding FEV1 and RV/TLC to GOLD or LLN improved the diagnostic accuracy, resulting in a significant reduction of up to 50% of the number of misdiagnoses. The expert diagnosis of COPD better predicts exacerbations, hospitalizations and mortality than GOLD or LLN.
Conclusions: GOLD criteria over-diagnose COPD, while LLN definitions under-diagnose COPD in elderly patients as compared to an expert panel diagnosis. Incorporating FEV1 and RV/TLC into the GOLD-COPD or LLN-based definition brings both definitions closer to expert panel diagnosis of COPD, and to daily clinical practice.
Figures
Comment in
-
GOLD or lower limit of normal definition? A letter and authors' response.Respir Res. 2012 Jul 26;13(1):61; author reply 61. doi: 10.1186/1465-9921-13-61. Respir Res. 2012. PMID: 22835077 Free PMC article. No abstract available.
Similar articles
-
COPD in chronic heart failure: less common than previously thought?Heart Lung. 2013 Sep-Oct;42(5):365-71. doi: 10.1016/j.hrtlng.2013.07.002. Heart Lung. 2013. PMID: 23998385
-
Vital capacity and COPD: the Swedish CArdioPulmonary bioImage Study (SCAPIS).Int J Chron Obstruct Pulmon Dis. 2016 May 2;11:927-33. doi: 10.2147/COPD.S104644. eCollection 2016. Int J Chron Obstruct Pulmon Dis. 2016. PMID: 27194908 Free PMC article.
-
Fixed ratio or lower limit of normal for the FEV1 /VC ratio: relation to symptoms and extended lung function tests.Clin Physiol Funct Imaging. 2017 May;37(3):263-269. doi: 10.1111/cpf.12294. Epub 2015 Oct 6. Clin Physiol Funct Imaging. 2017. PMID: 26443700
-
Lower limit of normal or FEV1/FVC < 0.70 in diagnosing COPD: an evidence-based review.Respir Med. 2011 Jun;105(6):907-15. doi: 10.1016/j.rmed.2011.01.008. Epub 2011 Feb 5. Respir Med. 2011. PMID: 21295958 Review.
-
What defines abnormal lung function in older adults with chronic obstructive pulmonary disease?Drugs Aging. 2008;25(9):717-28. doi: 10.2165/00002512-200825090-00001. Drugs Aging. 2008. PMID: 18729545 Review.
Cited by
-
Modelling the dynamics of expiratory airflow to describe chronic obstructive pulmonary disease.Med Biol Eng Comput. 2014 Dec;52(12):997-1006. doi: 10.1007/s11517-014-1202-6. Epub 2014 Sep 30. Med Biol Eng Comput. 2014. PMID: 25266260
-
Voluntary pulmonary function screening with GOLD standard: an effective and simple approach to detect lung obstruction.J Thorac Dis. 2015 Nov;7(11):1970-7. doi: 10.3978/j.issn.2072-1439.2015.11.20. J Thorac Dis. 2015. PMID: 26716035 Free PMC article.
-
Overdiagnosis across medical disciplines: a scoping review.BMJ Open. 2017 Dec 27;7(12):e018448. doi: 10.1136/bmjopen-2017-018448. BMJ Open. 2017. PMID: 29284720 Free PMC article.
-
A mathematical reason for FEV1/FVC dependence on age.Respir Res. 2012 Jul 4;13(1):57. doi: 10.1186/1465-9921-13-57. Respir Res. 2012. PMID: 22762777 Free PMC article.
-
Estimating prevalence of chronic obstructive pulmonary disease in the Southern Cone of Latin America: how different spirometric criteria may affect disease burden and health policies.BMC Pulm Med. 2017 Dec 11;17(1):187. doi: 10.1186/s12890-017-0537-9. BMC Pulm Med. 2017. PMID: 29228947 Free PMC article.
References
-
- Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P, Fukuchi Y, Jenkins C, Rodriguez-Roisin R, van Weel C, Zielinski J. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. doi: 10.1164/rccm.200703-456SO. - DOI - PubMed
-
- Swanney MP, Ruppel G, Enright PL, Pedersen OF, Crapo RO, Miller MR, Jensen RL, Falaschetti E, Schouten JP, Hankinson JL, Stocks J, Quanjer PH. Using the lower limit of normal for the FEV1/FVC ratio reduces the misclassification of airway obstruction. Thorax. 2008;63(12):1046–1051. doi: 10.1136/thx.2008.098483. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
