

Systemic air embolism during percutaneous core needle biopsy of the lung: frequency and risk factors
- PMID: 22309812
- PMCID: PMC3608336
- DOI: 10.1186/1471-2466-12-2
Systemic air embolism during percutaneous core needle biopsy of the lung: frequency and risk factors
Abstract
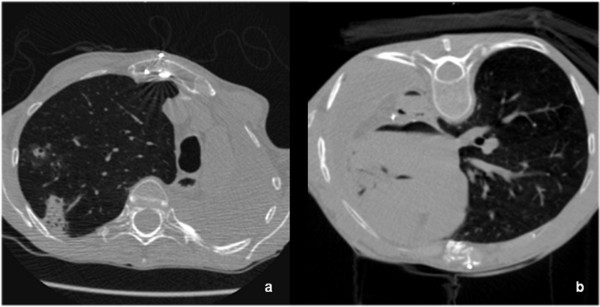
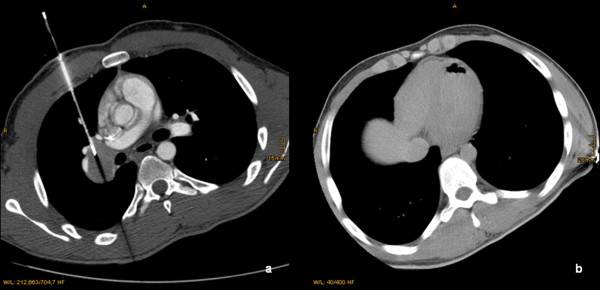
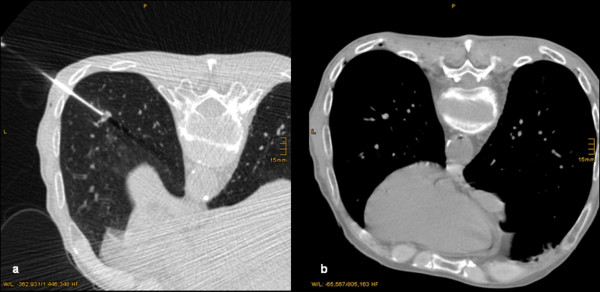
Background: Detection of risk factors for an air embolism in the left atrium, left ventricle, or systemic circulation (systemic air embolism, SAE) during a percutaneous core needle biopsy (PCNB) of the thorax.
Methods: In a retrospective observational study, all PCNBs of the thorax in 610 patients between 2007 and 2009 were analyzed. The SmartStep™ technique (General Electric) was used for the biopsy, with which the examiner can prepare a batch of three 1.25-mm or 2.5-mm collimated slices within a second using a foot switch in the CT room to check the needle position. The image data thus generated and the control CT scans that followed were examined retrospectively for the presence of intravascular air. Intravascular air was defined as two or more adjacent voxels with absorption values of < -200 HU in the left atrium, left ventricle, aorta, or arteries during or after the procedure. The univariate statistical analysis of categorical variables was made using 2 by 2 tables and the Fisher test. The groups were compared using the Mann-Whitney test. Finally, a multivariate logistic regression analysis was used to identify independent risk factors for the occurrence of an SAE.
Results: The radiological incidence of an SAE during a PCNB was 3.8% (23/610 patients), whereas the clinically apparent incidence was 0.49%. Two patients developed clinical symptoms consisting of transient hemiplegia or transient amaurosis; one died due to a fatal SAE of the coronary arteries. The mortality was thus 0.16%. The depth of the needle in the lesion (Wald: 6.859), endotracheal anesthesia (Wald: 5.721), location of the lesion above the level of the left atrium (Wald: 5.159), and prone position of the patients (Wald: 4.317) were independent risk factors for the incidence of an SAE (p < 0.05 each). Using explorative criteria, the acute angle of the needle to the tumor surface, and the transition of ventilated lung were independent factors. The frequency of biopsies, needle penetration depth, and tumor location near the diaphragm or in the lower lobe also played a subordinate role, not however, the needle penetration depth through the lung.
Conclusion: If possible, the PCNB should be performed under local anesthesia. We recommend avoiding endotracheal anesthesia and prone position. Whenever possible, patients should be positioned on the back in such a way that the tumor is lower than the left atrium. The tip of the needle should be within the tumor during the biopsy procedure.
Figures
References
-
- Lucidarme O, Howarth N, Finet JF, Grenier PA. Intrapulmonary lesions: percutaneous automated biopsy with a detachable, 18-gauge, coaxial cutting needle. Radiology. 1998;207:759–765. - PubMed
-
- Richardson CM, Pointon KS, Manhire AR, Macfarlane JT. Percutaneous lung biopsies: a survey of UK practice based on 5444 biopsies. Br J Radiol. 2002;75:731–735. - PubMed
-
- Tomiyama N, Yasuhara Y, Nakajima Y, Adachi S, Arai Y, Kusumoto M, Eguchi K, Kuriyama K, Sakai F, Noguchi M, Murata K, Murayama S, Mochizuki T, Mori K, Yamada K. CT-guided needle biopsy of lung lesions: a survey of severe complication based on 9783 biopsies in Japan. Eur J Radiol. 2006;59:60–64. doi: 10.1016/j.ejrad.2006.02.001. - DOI - PubMed
-
- Sinner WH. The value and use of percutaneous trans-thoracic needle biopsy in the diagnosis of intra-thoracic disease. Technique, indications, results and complications. Röfo. 1975;123:197–202. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
