

Unique pattern of complications in elderly trauma patients at a Level I trauma center
- PMID: 22310124
- PMCID: PMC3836632
- DOI: 10.1097/TA.0b013e318241f073
Unique pattern of complications in elderly trauma patients at a Level I trauma center
Abstract
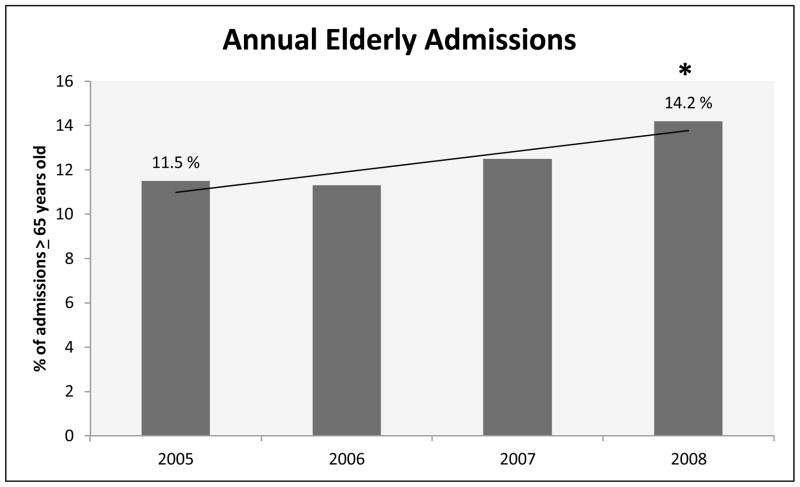
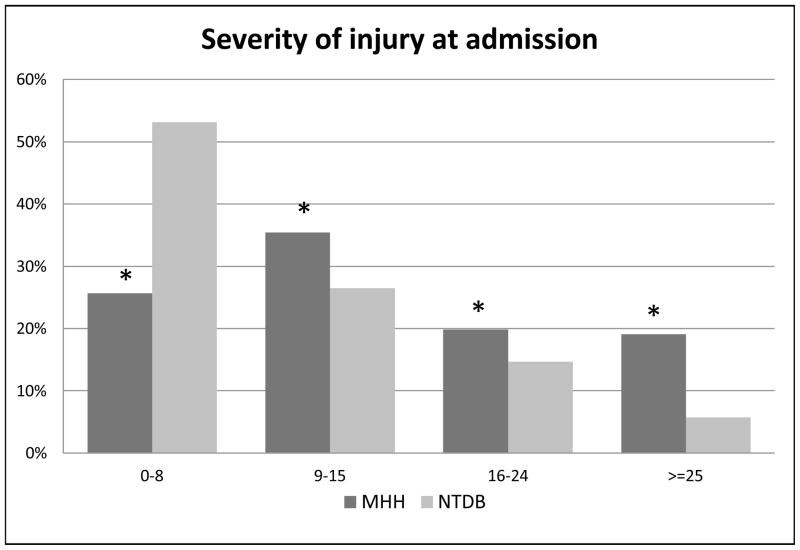
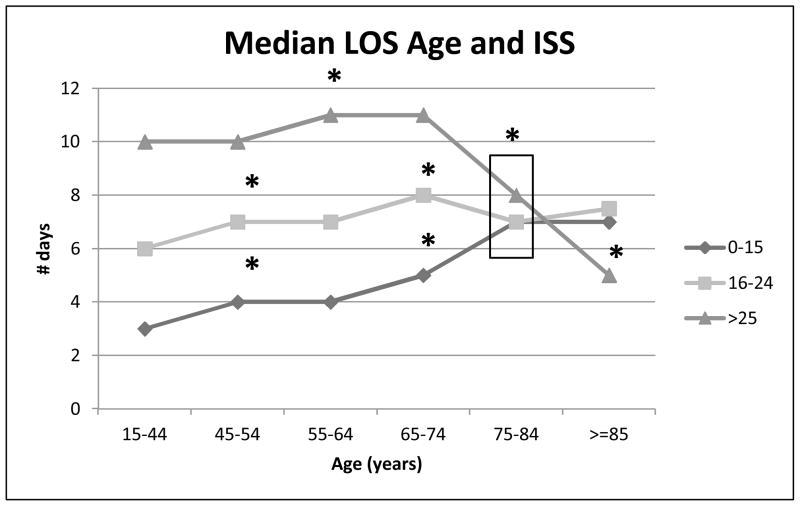
Background: Trauma centers are caring for increased proportions of elderly patients. Although age and Injury Severity Score are independently associated with mortality, trauma centers were originally designed to care for seriously injured patients without age-specific guidelines. We hypothesized that elderly patients would have different complication patterns than their younger counterparts.
Methods: The trauma registry of an American College of Surgeons -verified Level I trauma center was queried for all patients older than 14 years admitted between January 2005 and December 2008. Mechanism, mortality, and complications were evaluated after dividing patients into eight age groups.
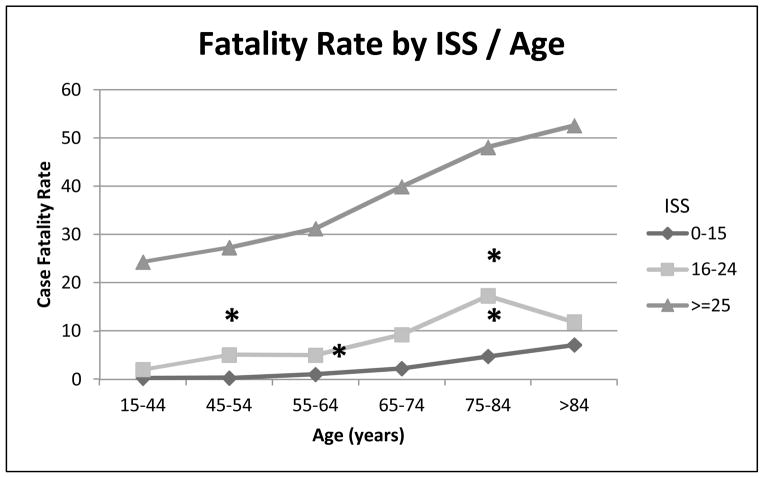
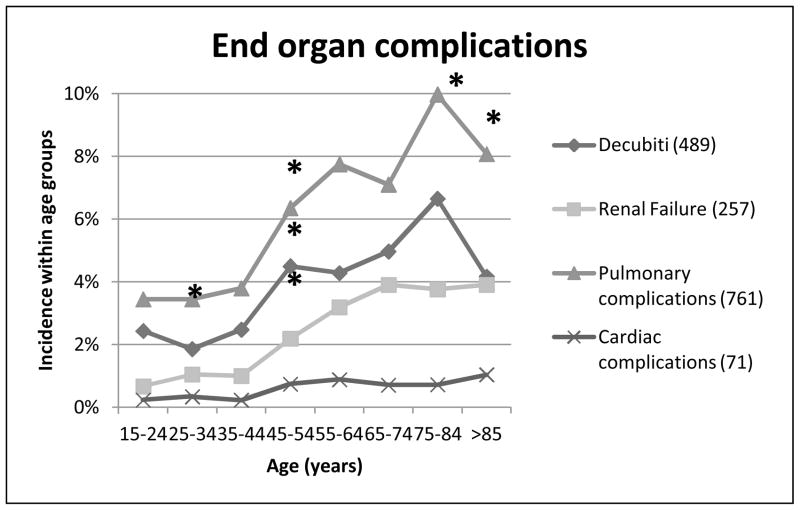
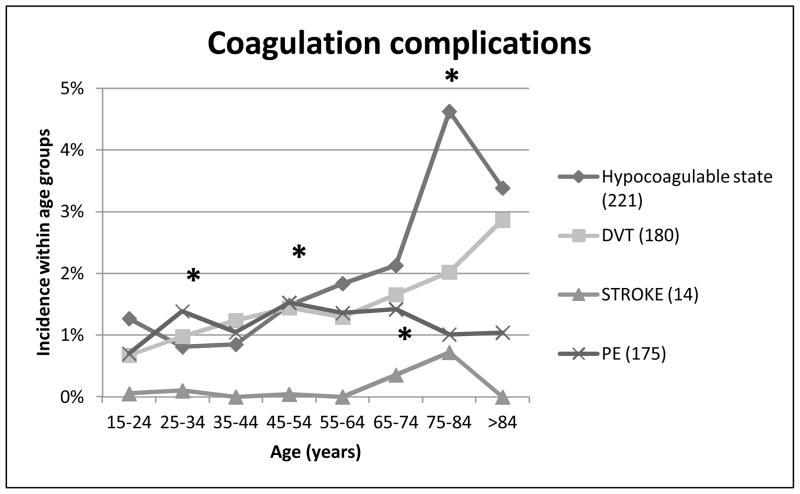
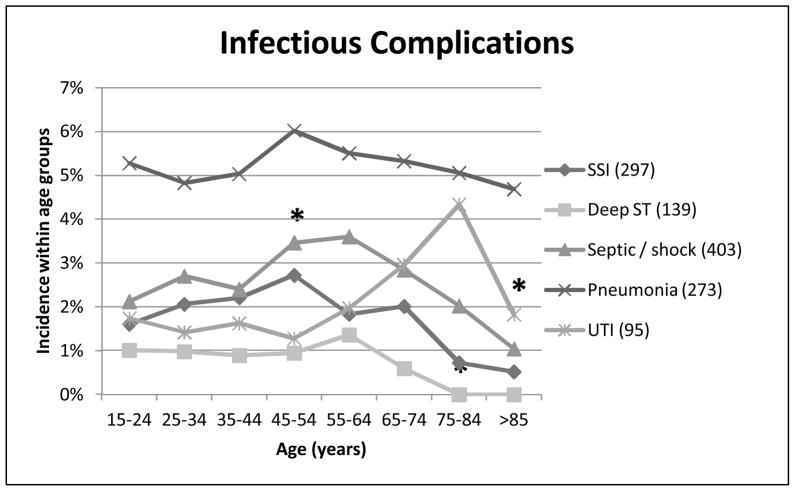
Results: Of the 15,223 patients, 13% were elderly (≥65), and 86% were injured via a blunt mechanism. Increasing age correlated with fatality (all Injury Severity Scores), end-organ failure, and thromboembolic complications (deep venous thrombosis and coagulopathy). Analysis revealed a significant breakpoint at 45 years of age for mortality, decubitus ulcer, and renal failure (all p values <0.05). Infectious complications (sepsis, wound infection, and abscess) all peaked between 45 years and 65 years and then declined with increasing age.
Conclusions: We document that elderly trauma patients suffer the same complications as their younger counterparts, albeit at a different rate. More importantly, we identified a "breakpoint" of increased risk of complications and mortality at greater than 45 years. Although the mechanisms behind these observations remain unknown, understanding their unique patterns may allow appropriate allocation of resources and focus research efforts on interventions that should improve outcomes.
Figures
References
-
- U.S. Census Bureau. Population estimates. http://www.census.gov/popest/estimates.html.
-
- Tornetta P, 3rd, Mostafavi H, Riina J, et al. Morbidity and mortality in elderly trauma patients. J Trauma. 1999;46(4):702–6. - PubMed
-
- Taylor MD, Tracy JK, Meyer W, et al. Trauma in the elderly: intensive care unit resource and outcome. J Trauma. 2002;53(3):407–14. - PubMed
-
- Newell MA, Rotondo MF, Toschlog EA, et al. The elderly trauma patient: An investment for the future? J Trauma. 2009;67(2):337–340. - PubMed
-
- Potoka DA, Schall LC, Gardner MJ, et al. Impact of pediatric trauma centers on mortality in a statewide system. J Trauma. 2000;49(2):237–45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
