

Prior antiarrhythmic drug use and the outcome of atrial fibrillation ablation
- PMID: 22310154
- PMCID: PMC4051413
- DOI: 10.1093/europace/eur370
Prior antiarrhythmic drug use and the outcome of atrial fibrillation ablation
Abstract
Aims: Atrial fibrillation (AF) ablation is generally performed after patients fail antiarrhythmic drug (AAD) therapy. Some patients have drug contraindications or choose to avoid a lifetime of drug therapy. Little is known about the impact of previous drug therapy on ablation outcomes. We evaluated AAD use before AF ablation and its impact on ablation outcomes.
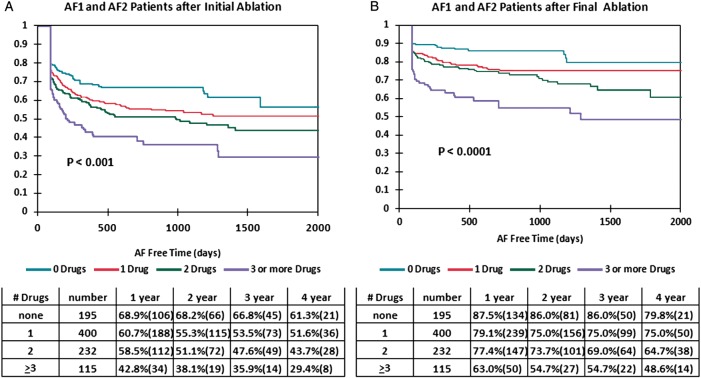
Methods and results: We evaluated freedom from AF after ablation and patients' clinical characteristics by number of AADs failed in 1125 patients undergoing 1504 ablations. We also evaluated reasons why some patients did not receive prior drug therapy. Cox multivariate analysis examined factors predicting ablation failure. Patients failing more drugs before ablation were older (P = 0.001), had a longer duration of AF (P = 0.0001), were more likely female (P = 0.037), had more repeat ablations (P = 0.045), and less paroxysmal AF (P = 0.003). For patients with either paroxysmal or persistent AF, the number of drugs failed predicted AF recurrence (P = 0.0001). Other factors predicting AF recurrence following final ablation included age (P = 0.004), left atrial size (P = 0.002), female gender (P = 0.0001), and persistent AF (P = 0.0001). The reason for not receiving prior drug therapy was medical in 21.5% and patient choice in 78.5%. Number of drugs failed did not influence ablation outcome for patients with long-standing persistent AF (P = 0.352).
Conclusions: For paroxysmal and persistent AF patients undergoing ablation, those failing fewer AADs have different clinical characteristics than those who fail more drugs. Our study also suggests that the more drugs failed pre-ablation, the lower the freedom from AF post-procedure, possibly due to AF progression during drug trials.
Figures
Comment in
-
Atrial fibrillation: is there evidence to support an early ablation strategy?Europace. 2012 May;14(5):613-4. doi: 10.1093/europace/eus008. Epub 2012 Feb 6. Europace. 2012. PMID: 22310152 No abstract available.
References
-
- Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: full text: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 guidelines for the management of patients with atrial fibrillation) developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Europace. 2006;8:651–745. - PubMed
-
- Calkins H, Brugada J, Packer DL, Capppato R, Chen S, Crijns H, et al. HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. Europace. 2007;9:335–79. - PubMed
-
- Wann LS, Curtis AB, January CT, Ellenbogen KA, Lowe JE, Estes NAM, et al. ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation updating the 2006 guideline) Heart Rhythm. 2011;8:157–76. - PubMed
-
- Camm AJ, Kirchhof P, Lip GYJ, Schotten U, Savelieva I, Ernst S, et al. Guidelines for the management of atrial fibrillation. Eur Heart J. 2010;31:2369–429. - PubMed
-
- Verma A, Macle L, Cos J, Skanes AC. Canadian cardiovascular society atrial fibrillation guidelines 2010: catheter ablation for atrial fibrillation/atrial flutter. Can J Cardiol. 2011;27:60–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
