

Implications of Identifying Additional Cerebral Metastases during Gamma Knife Radiosurgery
- PMID: 22312543
- PMCID: PMC3265271
- DOI: 10.1155/2012/748284
Implications of Identifying Additional Cerebral Metastases during Gamma Knife Radiosurgery
Abstract
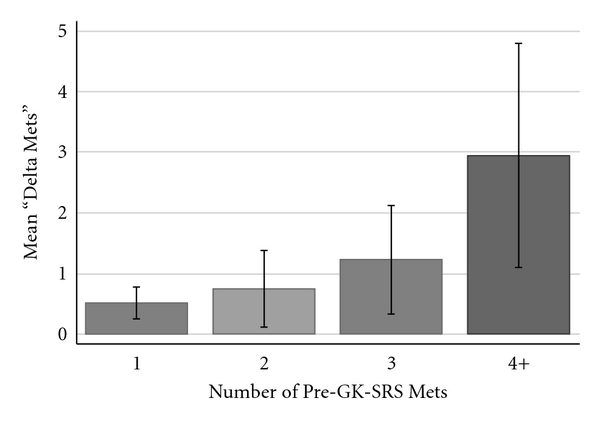
Introduction. Gamma Knife radiosurgery (GK-SRS) is commonly used to treat cerebral metastases. Although additional intracranial metastases are often found on the day of GK-SRS, the significance of finding them is unknown. Methods. A retrospective review of 133 patients undergoing GK-SRS for cerebral metastases was performed. The change in number of metastases detected between initial referral magnetic resonance imaging (MRI) and subsequent treatment MRI was quantified. Multivariate and Kaplan-Meier analyses were employed to examine the significance of identifying additional lesions. Results. Additional lesions were identified in 41% of patients. An increasing number of metastases on referral MRI (P = 0.001) and the presence of progressive systemic disease (P = 0.003) were predictive of identifying additional metastases. Median survival was 6.9 months for patients with additional metastases, compared to 12.1 months for patients without additional metastases (hazard ratio 1.56, P = 0.021). Conclusions. Identifying additional metastases on the day of GK-SRS may add important prognostic information.
Figures



References
-
- Kim SH, Weil RJ, Chao ST, et al. Stereotactic radiosurgical treatment of brain metastases in older patients. Cancer. 2008;113(4):834–840. - PubMed
-
- Nussbaum ES, Djalilian HR, Cho KH, Hall WA. Brain metastases: histology, multiplicity, surgery, and survival. Cancer. 1996;78(8):1781–1788. - PubMed
-
- Sperduto CM, Watanabe Y, Mullan J, et al. A validation study of a new prognostic index for patients with brain metastases: the graded prognostic assessment. Journal of Neurosurgery. 2008;109:87–89. - PubMed
-
- Chao ST, Barnett GH, Liu SW, et al. Five-year survivors of brain metastases: a single-institution report of 32 patients. International Journal of Radiation Oncology Biology Physics. 2006;66(3):801–809. - PubMed
LinkOut - more resources
Full Text Sources
