

A role for cytomegalovirus-specific CD4+CX3CR1+ T cells and cytomegalovirus-induced T-cell immunopathology in HIV-associated atherosclerosis
- PMID: 22313962
- PMCID: PMC4155398
- DOI: 10.1097/QAD.0b013e328351f780
A role for cytomegalovirus-specific CD4+CX3CR1+ T cells and cytomegalovirus-induced T-cell immunopathology in HIV-associated atherosclerosis
Abstract
Objective: HIV-infected individuals are at increased risk for myocardial infarction. Given observations that cytomegalovirus (CMV) infection, CMV-specific T cells, and CX3CR1 have each been associated with atherosclerosis, we hypothesized that CMV-induced T-cell immunopathology could contribute to HIV-associated atherosclerosis.
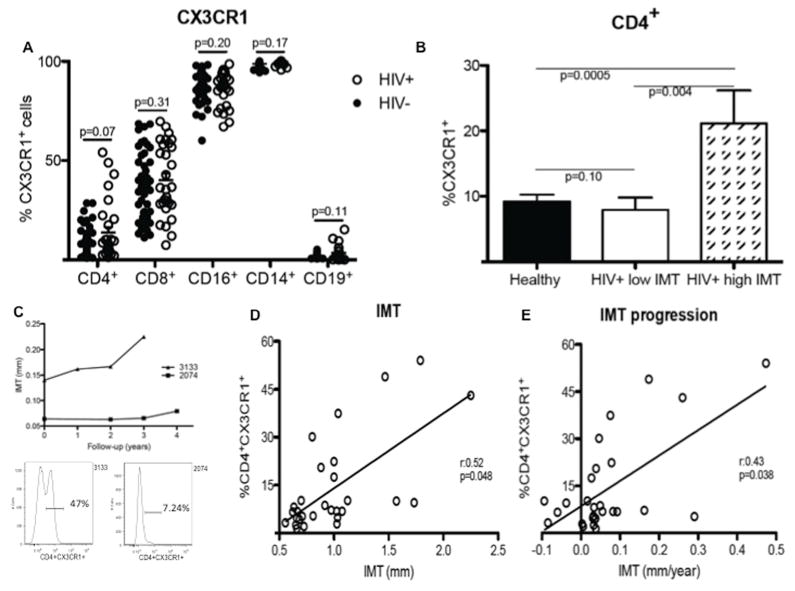
Methods: We measured the expression of CX3CR1 on peripheral blood mononuclear cells and its association with carotid artery intima-media thickness (IMT) in 29 HIV-infected individuals and 48 uninfected controls. We analyzed the phenotype and specificity of CX3CR1(+)CD4(+) T cells, the production of CX3CL1 (the ligand of CX3CR1) by CMV-infected endothelial cells in vitro, and the migration of CD4(+) T cells induced by CX3CL1.
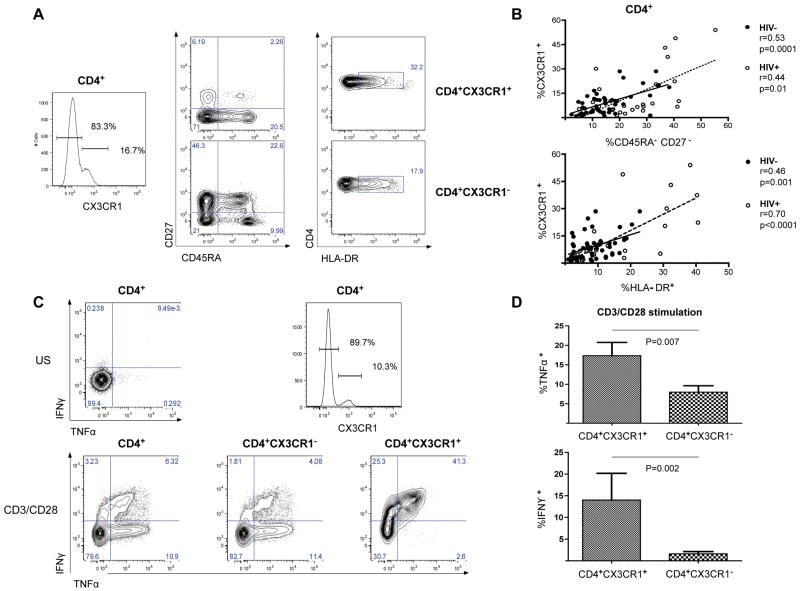
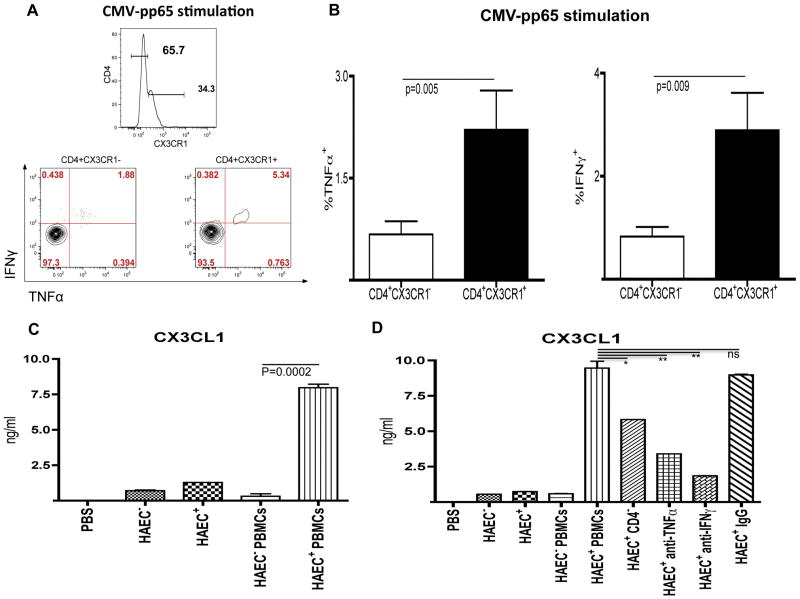
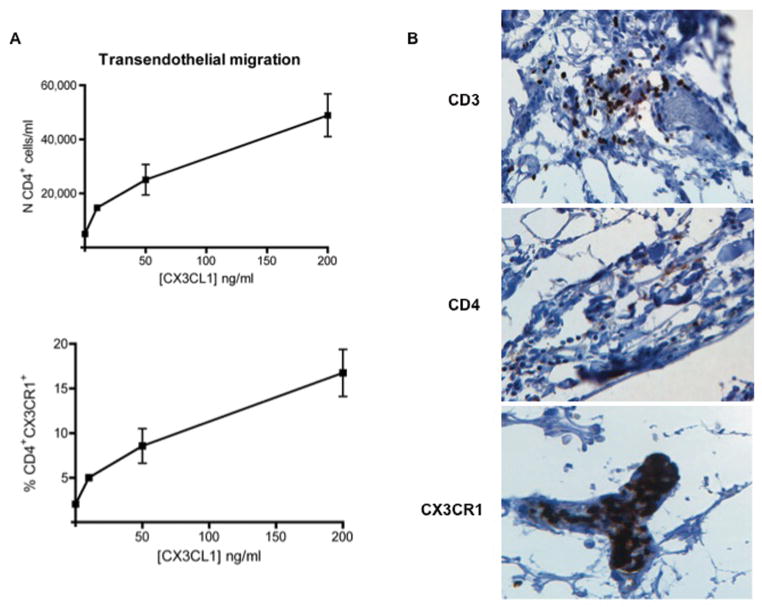
Results: The progression of atherosclerosis in HIV-infected individuals, as assessed by longitudinal measurements of carotid IMT, was associated with a high frequency of CD4(+) T cells that express the chemokine receptor CX3CR1. Such CD4(+)CX3CR1(+) T cells were antigen-primed, produced high levels of pro-inflammatory cytokines, and composed the majority of the CMV-specific CD4(+) T cells. CMV-stimulated CD4(+) T cells were also found to induce the production of CX3CL1 (the ligand for CX3CR1) by human arterial endothelial cells, driving the transendothelial migration of pro-inflammatory CD4(+) T cells. Finally, we observed that CD4(+)CX3CR1(+) T cells could be localized to the coronary arterial wall in HIV disease.
Conclusion: HIV-associated atherosclerosis may be driven by a positive feedback pathway in which a high frequency of antigen-stimulated, CMV-specific CD4(+)CX3CR1(+) T cells induce endothelial cells to secrete CX3CL1, which itself drives progressive infiltration of the arterial wall by pro-inflammatory cells.
Conflict of interest statement
There are no financial conflicts of interest associated with this work.
Figures
References
-
- Hsue PY, Lo JC, Franklin A, Bolger AF, Martin JN, Deeks SG, et al. Progression of atherosclerosis as assessed by carotid intima-media thickness in patients with HIV infection. Circulation. 2004;109:1603–1608. - PubMed
-
- Barbaro G, Fisher SD, Lipshultz SE. Pathogenesis of HIV-associated cardiovascular complications. Lancet Infect Dis. 2001;1:115–124. - PubMed
-
- Durand M, Sheehy O, Baril JG, Lelorier J, Tremblay CL. Association between HIV infection, antiretroviral therapy, and risk of acute myocardial infarction: a cohort and nested case-control study using Quebec’s public health insurance database. Journal of Acquired Immune Deficiency Syndromes. 2011;57:245–253. - PubMed
-
- van Vonderen MG, Hassink EA, van Agtmael MA, Stehouwer CD, Danner SA, Reiss P, et al. Increase in carotid artery intima-media thickness and arterial stiffness but improvement in several markers of endothelial function after initiation of antiretroviral therapy. The Journal of Infectious Diseases. 2009;199:1186–1194. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
