

Unresponsiveness ≠ unconsciousness
- PMID: 22314293
- PMCID: PMC3311716
- DOI: 10.1097/ALN.0b013e318249d0a7
Unresponsiveness ≠ unconsciousness
Abstract
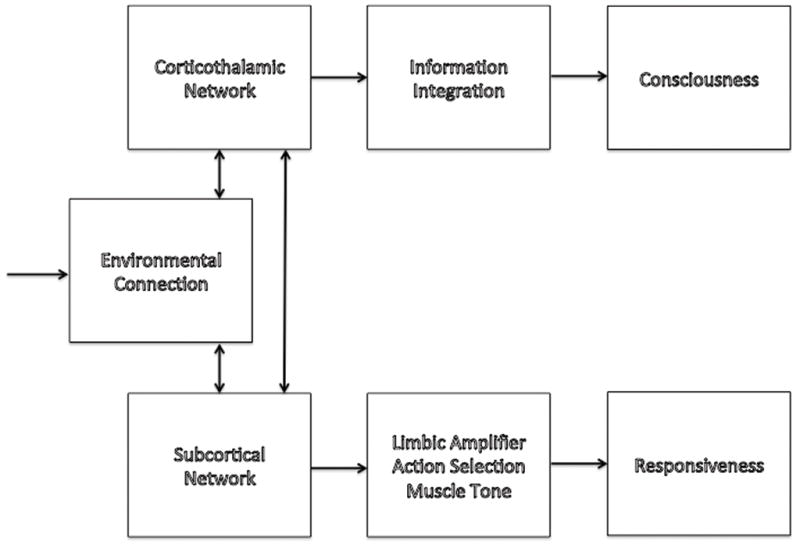
Consciousness is subjective experience. During both sleep and anesthesia, consciousness is common, evidenced by dreaming. A defining feature of dreaming is that, while conscious, we do not experience our environment; we are disconnected. Besides inducing behavioral unresponsiveness, a key goal of anesthesia is to prevent the experience of surgery (connected consciousness), by inducing either unconsciousness or disconnection of consciousness from the environment. Review of the isolated forearm technique demonstrates that consciousness, connectedness, and responsiveness uncouple during anesthesia; in clinical conditions, a median 37% of patients demonstrate connected consciousness. We describe potential neurobiological constructs that can explain this phenomenon: during light anesthesia the subcortical mechanisms subserving spontaneous behavioral responsiveness are disabled but information integration within the corticothalamic network continues to produce consciousness, and unperturbed norepinephrinergic signaling maintains connectedness. These concepts emphasize the need for developing anesthetic regimens and depth of anesthesia monitors that specifically target mechanisms of consciousness, connectedness, and responsiveness.
Conflict of interest statement
Conflict of Interest: RDS has received honoraria for speaking on behalf of Hospira, Illinois, USA. Hospira, or any other industry, had no input into design of the talk or this manuscript.
Figures


Comment in
-
Unresponsiveness versus unconsciousness.Anesthesiology. 2012 Nov;117(5):1140; author reply 1140. doi: 10.1097/ALN.0b013e31826f8b9a. Anesthesiology. 2012. PMID: 23095543 No abstract available.
References
-
- Seneca L. Letters from a Stoic: Epistulae Morales ad Lucilium. New York: Penguin Books; 1969.
-
- Tononi G, Laureys S. In: The Neurology of Consciousness: An Overview, The Neurology of Consciousness. 1. Laureys S, Tononi G, editors. London: Academic Press; 2009. pp. 375–412.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
