

Diagnosis of DVT: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines
- PMID: 22315267
- PMCID: PMC3278048
- DOI: 10.1378/chest.11-2299
Diagnosis of DVT: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines
Abstract
Background: Objective testing for DVT is crucial because clinical assessment alone is unreliable and the consequences of misdiagnosis are serious. This guideline focuses on the identification of optimal strategies for the diagnosis of DVT in ambulatory adults.
Methods: The methods of this guideline follow those described in Methodology for the Development of Antithrombotic Therapy and Prevention of Thrombosis Guidelines: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines.
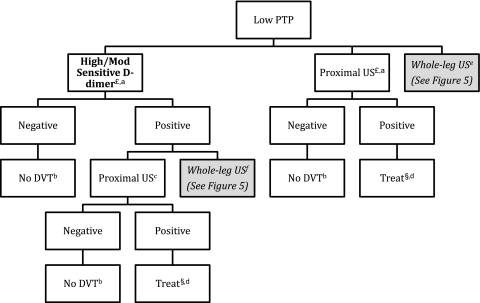
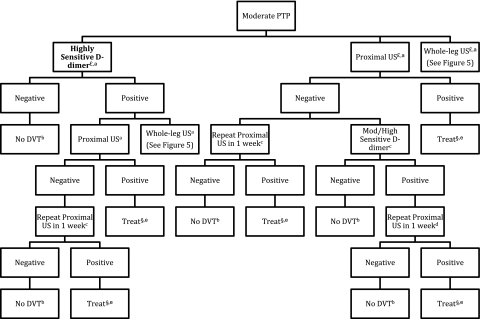
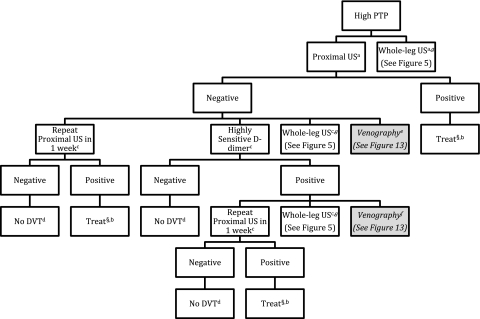
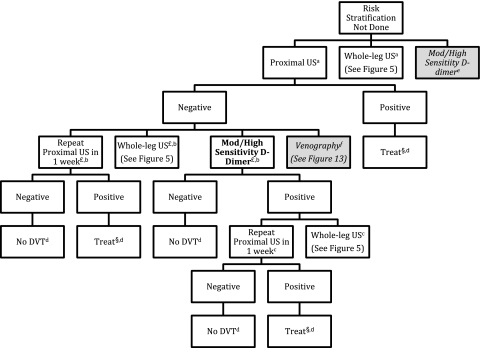
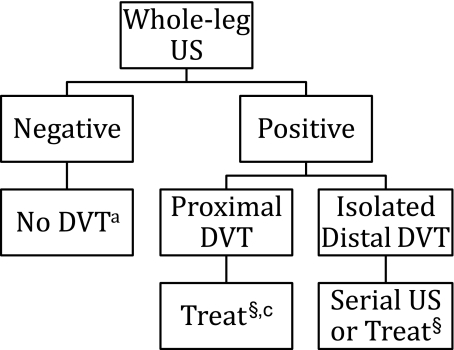
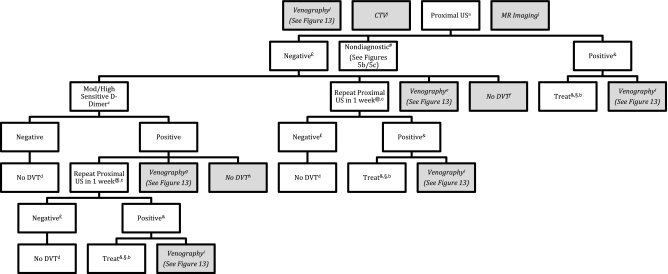
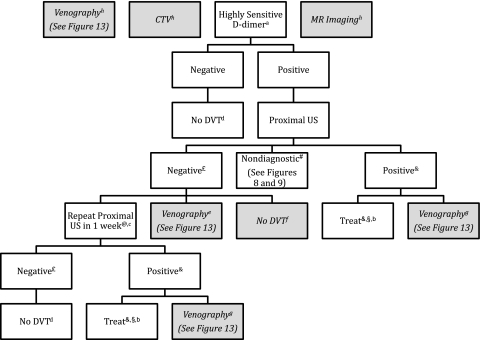
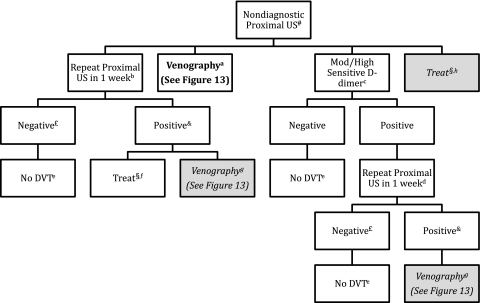
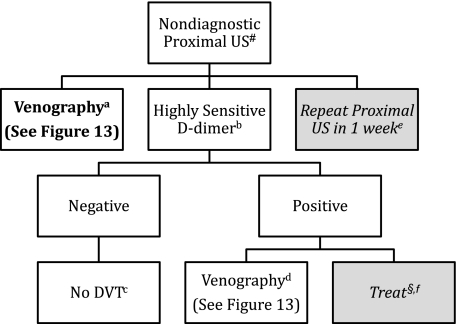
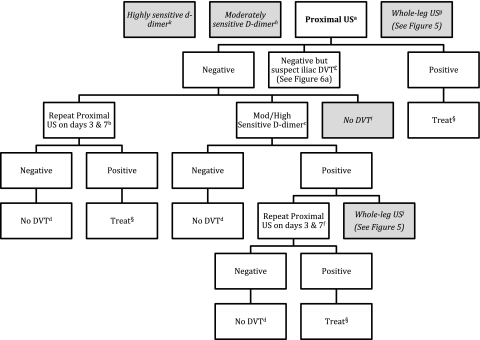
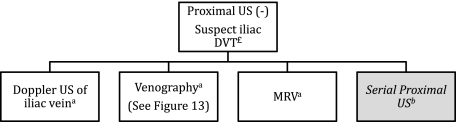
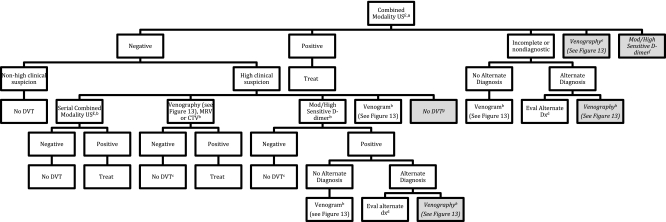
Results: We suggest that clinical assessment of pretest probability of DVT, rather than performing the same tests in all patients, should guide the diagnostic process for a first lower extremity DVT (Grade 2B). In patients with a low pretest probability of first lower extremity DVT, we recommend initial testing with D-dimer or ultrasound (US) of the proximal veins over no diagnostic testing (Grade 1B), venography (Grade 1B), or whole-leg US (Grade 2B). In patients with moderate pretest probability, we recommend initial testing with a highly sensitive D-dimer, proximal compression US, or whole-leg US rather than no testing (Grade 1B) or venography (Grade 1B). In patients with a high pretest probability, we recommend proximal compression or whole-leg US over no testing (Grade 1B) or venography (Grade 1B).
Conclusions: Favored strategies for diagnosis of first DVT combine use of pretest probability assessment, D-dimer, and US. There is lower-quality evidence available to guide diagnosis of recurrent DVT, upper extremity DVT, and DVT during pregnancy.
Figures
References
-
- Anderson FA, Jr, Wheeler HB, Goldberg RJ, et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med. 1991;151(5):933–938. - PubMed
-
- Silverstein MD, Heit JA, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ., III Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 1998;158(6):585–593. - PubMed
-
- McLachlin J, Richards T, Paterson JC. An evaluation of clinical signs in the diagnosis of venous thrombosis. Arch Surg. 1962;85:738–744. - PubMed
-
- Nicolaides AN, Kakkar VV, Field ES, Renney JT. The origin of deep vein thrombosis: a venographic study. Br J Radiol. 1971;44(525):653–663. - PubMed
-
- Sandler DA, Martin JF, Duncan JS, et al. Diagnosis of deep-vein thrombosis: comparison of clinical evaluation, ultrasound, plethysmography, and venoscan with X-ray venogram. Lancet. 1984;2(8405):716–719. - PubMed
