

Bone marrow versus peripheral blood as the stem cell source for sibling transplants in acquired aplastic anemia: survival advantage for bone marrow in all age groups
- PMID: 22315497
- PMCID: PMC3409810
- DOI: 10.3324/haematol.2011.054841
Bone marrow versus peripheral blood as the stem cell source for sibling transplants in acquired aplastic anemia: survival advantage for bone marrow in all age groups
Abstract
Background: Bone marrow has been shown to be superior to peripheral blood, as a stem cell source, in young patients (<20 years of age) with acquired aplastic anemia undergoing a matched sibling transplant. The aim of this study was to test whether this currently also holds true for older patients with acquired aplastic anemia.
Design and methods: We analyzed 1886 patients with acquired aplastic anemia who received a first transplant from a human leukocyte antigen identical sibling between 1999 and 2009, with either bone marrow (n=1163) or peripheral blood (n=723) as the source of stem cells.
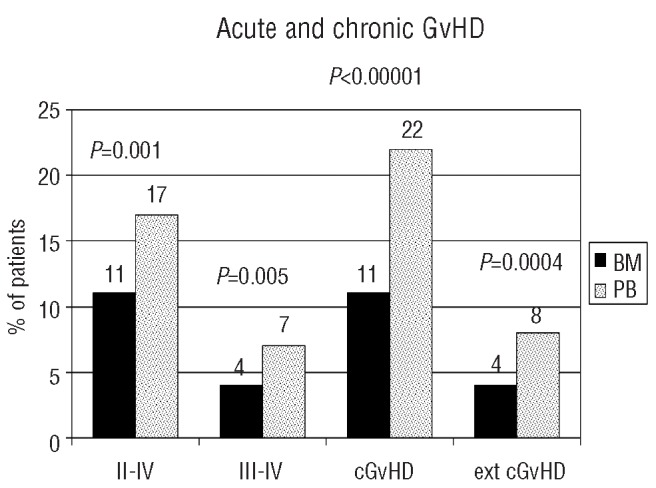
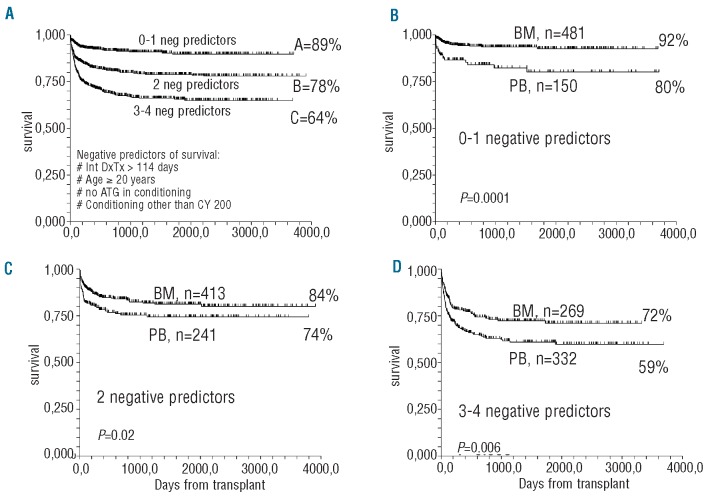
Results: In multivariate Cox analysis negative predictors for survival were: patient's age over 20 years (RR 2.0, P<0.0001), an interval between diagnosis and transplantation of more than 114 days (RR 1.3, P=0.006), no anti-thymocyte globulin in the conditioning (RR 1.6, P=0.0001), a conditioning regimen other than cyclophosphamide (RR=1.3, P=0.008) and the use of peripheral blood as the source of stem cells (RR 1.6, P<0.00001). The survival advantage for recipients of bone marrow rather than peripheral blood was statistically significant in patients aged 1-19 years (90% versus 76% P<0.00001) as well as in patients aged over 20 years (74% versus 64%, P=0.001). The advantage for recipients of bone marrow over peripheral blood was maintained above the age of 50 years (69% versus 39%, P=0.01). Acute and chronic graft-versus-host disease were more frequent in peripheral blood transplants. Major causes of death were graft-versus-host disease (2% versus 6% in bone marrow and peripheral blood recipients, respectively), infections (6% versus 13%), and graft rejection (1.5% versus 2.5%).
Conclusions: This study shows that bone marrow should be the preferred stem cell source for matched sibling transplants in acquired aplastic anemia, in patients of all age groups.
Figures


References
-
- Storb R, Thomas ED, Buckner CD, Clift RA, Johnson FL, Fefer A, et al. Allogeneic marrow grafting for treatment of aplastic anemia. Blood. 1974;43(2):157–80. - PubMed
-
- Schrezenmeier H, Passweg JR, Marsh JC, Bacigalupo A, Bredeson CN, Bullorsky E, et al. Worse outcome and more chronic GVHD with peripheral blood progenitor cells than bone marrow in HLA-matched sibling donor transplants for young patients with severe acquired aplastic anemia. Blood. 2007;110(4):1397–400. - PMC - PubMed
-
- Chu R, Brazauskas R, Kan F, Bashey A, Bredeson C, Camitta B, et al. Comparison of outcomes after transplantation of G-CSF-stimulated bone marrow grafts versus bone marrow or peripheral blood grafts from HLA-matched sibling donors for patients with severe aplastic anemia. Biol Blood Marrow Transplant. 2011;17(7):1018–24. - PMC - PubMed
-
- Friedrichs B, Tichelli A, Bacigalupo A, Russell NH, Ruutu T, Shapira MY, et al. Long-term outcome and late effects in patients transplanted with mobilised blood or bone marrow: a randomised trial. Lancet Oncol. 2010;11(4):331–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
