

Crohn's disease imaging: a review
- PMID: 22315589
- PMCID: PMC3270553
- DOI: 10.1155/2012/816920
Crohn's disease imaging: a review
Abstract
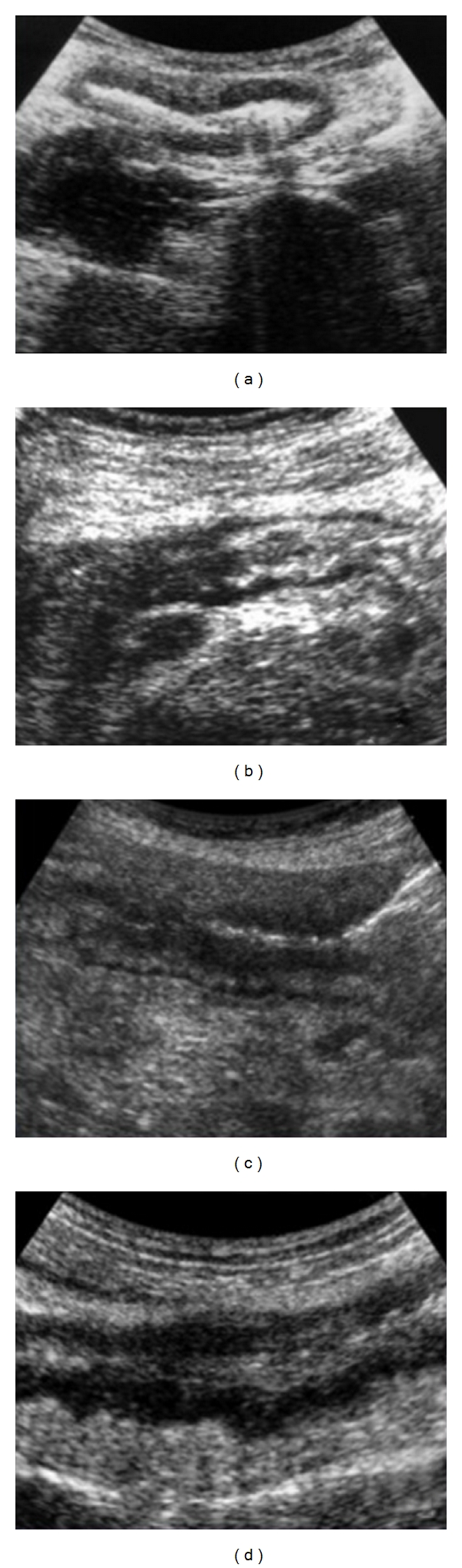
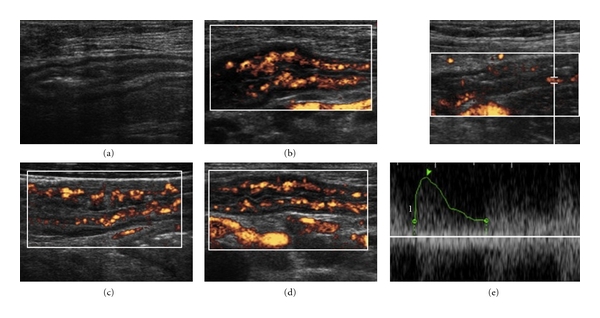
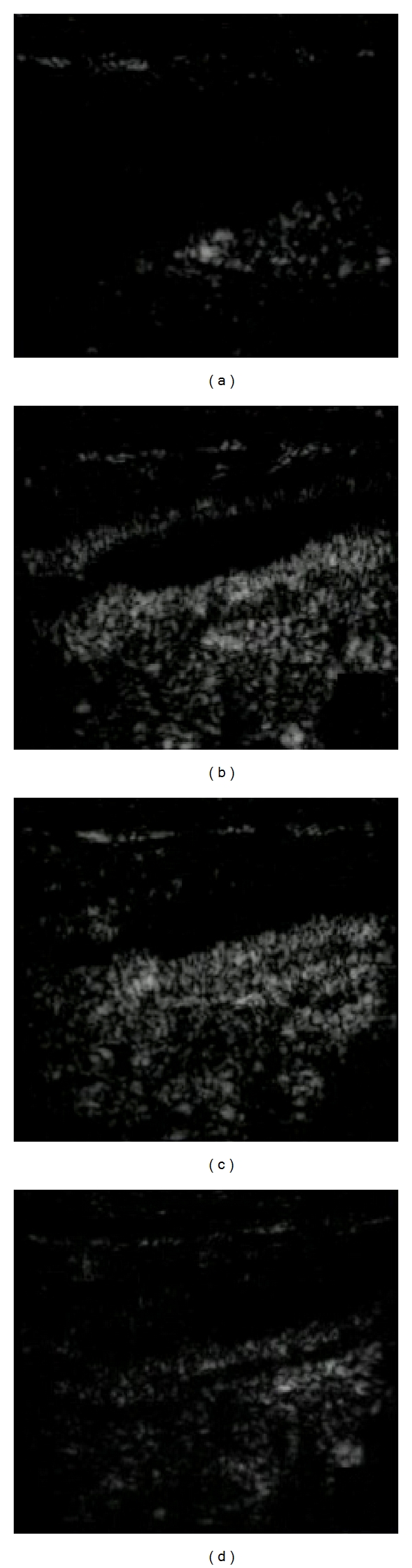
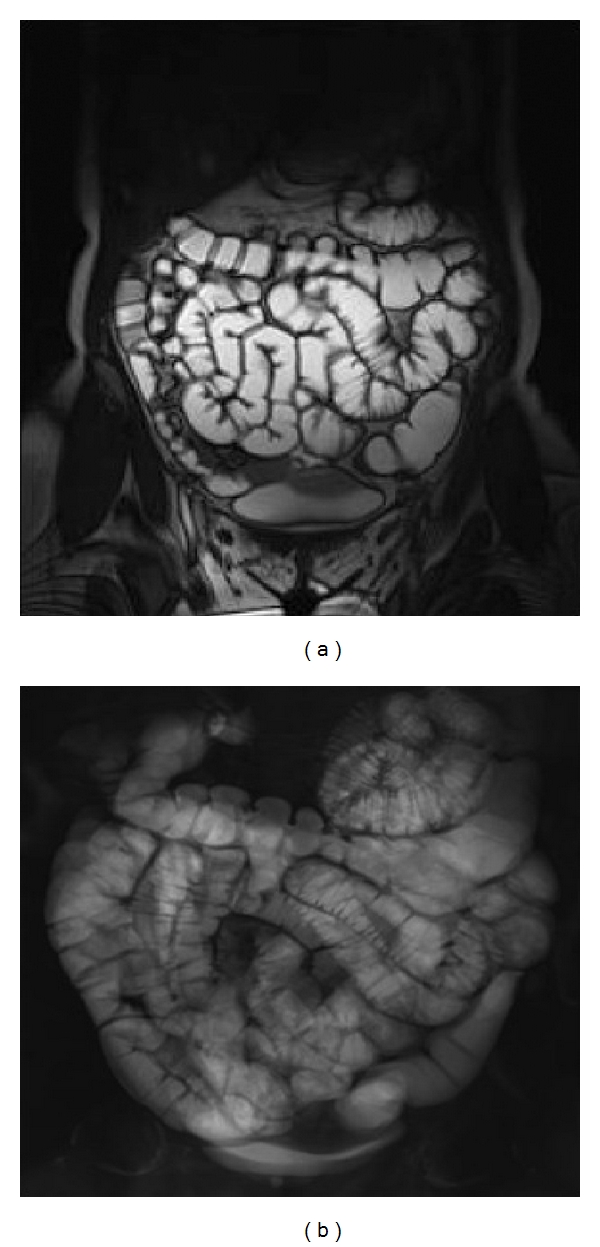
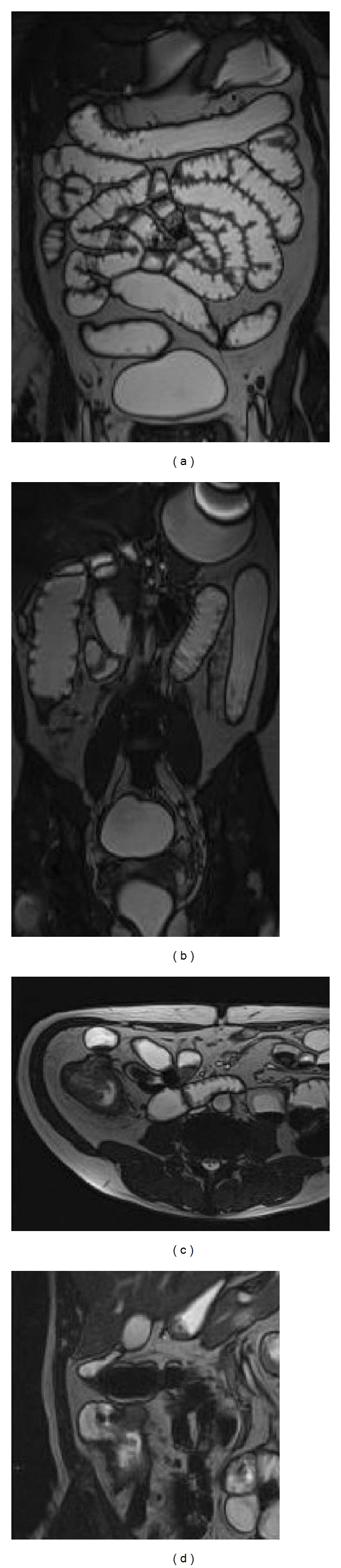
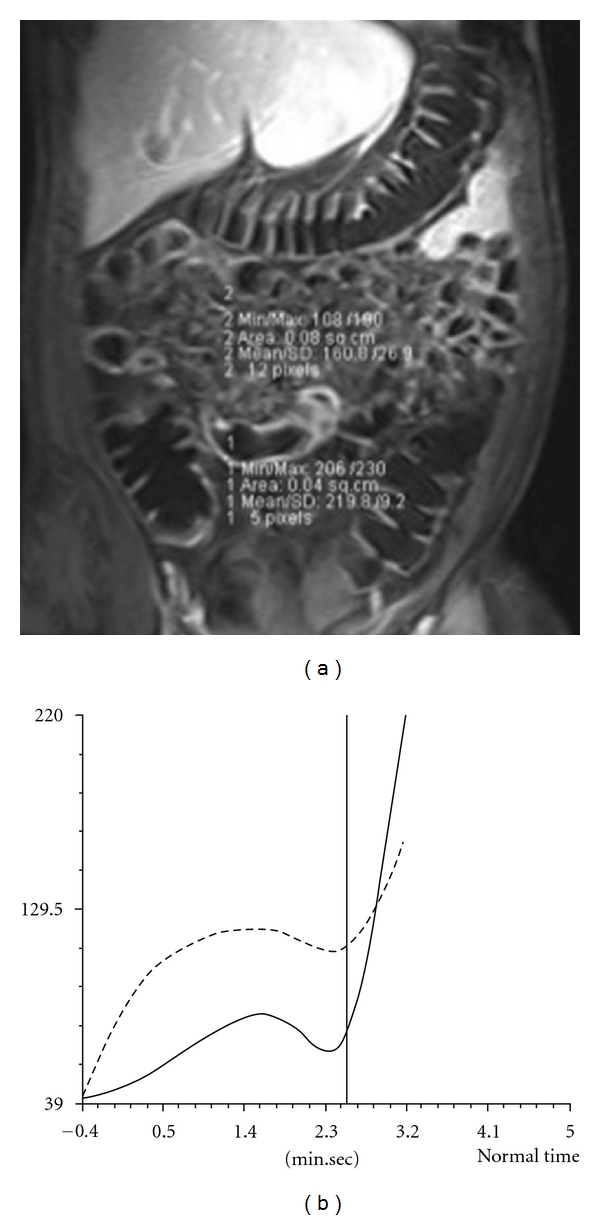
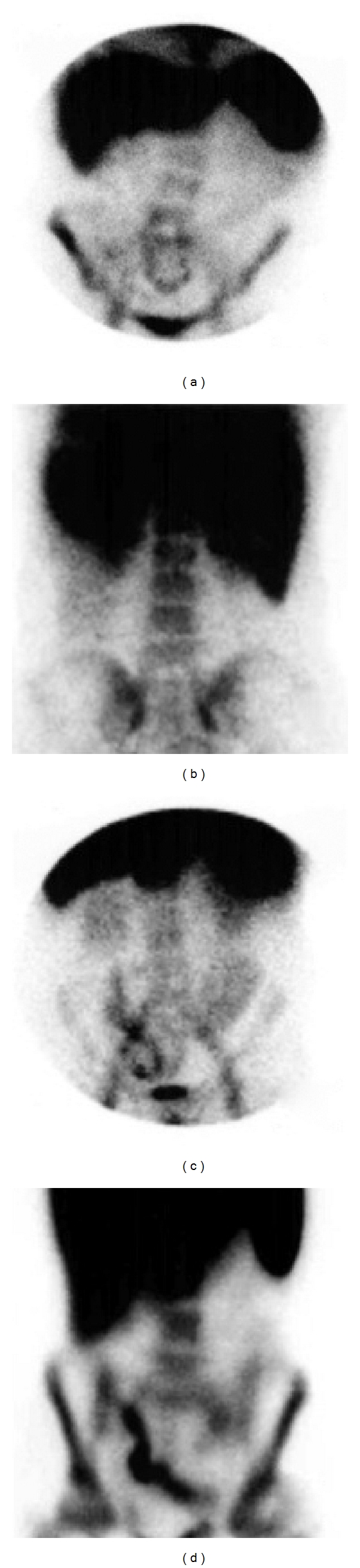
Crohn's disease is a chronic granulomatous inflammatory disease of the gastrointestinal tract, which can involve almost any segment from the mouth to the anus. Typically, Crohn's lesions attain segmental and asynchronous distribution with varying levels of seriousness, although the sites most frequently involved are the terminal ileum and the proximal colon. A single gold standard for the diagnosis of CD is not available and the diagnosis of CD is confirmed by clinical evaluation and a combination of endoscopic, histological, radiological, and/or biochemical investigations. In recent years, many studies have been performed to investigate the diagnostic potential of less invasive and more patient-friendly imaging modalities in the evaluation of Crohn's disease including conventional enteroclysis, ultrasonography, color-power Doppler, contrast-enhanced ultrasonography, multidetector CT enteroclysis, MRI enteroclysis, and 99mTc-HMPAO-labeled leukocyte scintigraphy. The potential diagnostic role of each imaging modality has to be considered in different clinical degrees of the disease, because there is no single imaging technique that allows a correct diagnosis and may be performed with similar results in every institution. The aim of this paper is to point out the advantages and limitations of the various imaging techniques in patients with suspected or proven Crohn's disease.
Figures



References
-
- Herlinger H. A modified technique for the double-contrast small bowel enema. Gastrointestinal Radiology. 1978;3(2):201–207. - PubMed
-
- Maglinte DDT, Gage SN, Harmon BH, et al. Obstruction of the small intestine: accuracy and role of CT in diagnosis. Radiology. 1993;188(1):61–64. - PubMed
-
- Maconi G, Sanpietro GM, Parente F, et al. Contrastradiology, computed tomography and ultrasonography in detecting internal fistulas and intra-abdominal abscesses in Crohn’s disease: a prospective comparative study. The American Journal of Gastroenterology. 2003;98(7):1545–1555. - PubMed
-
- Glick SN. Crohn’s disease of the small intestine: accuracy and relevance of enteroclysis. Radiologic Clinics of North America. 1987;25:25–43. - PubMed
-
- Fraser GM, Findlay JM. The double contrast enema in ulcerative and Crohn’s colitis. Clinical Radiology. 1976;27(1):103–112. - PubMed
LinkOut - more resources
Full Text Sources
