Computed tomography findings in xanthogranulomatous pyelonephritis
- PMID: 22315712
- PMCID: PMC3272912
- DOI: 10.4103/2156-7514.84323
Computed tomography findings in xanthogranulomatous pyelonephritis
Abstract
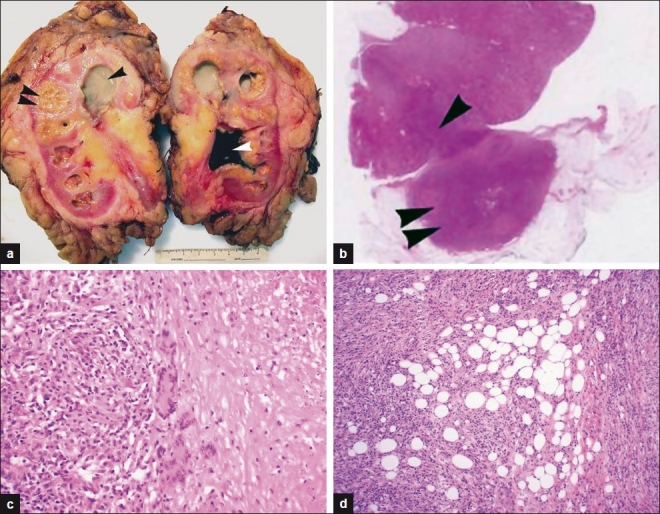
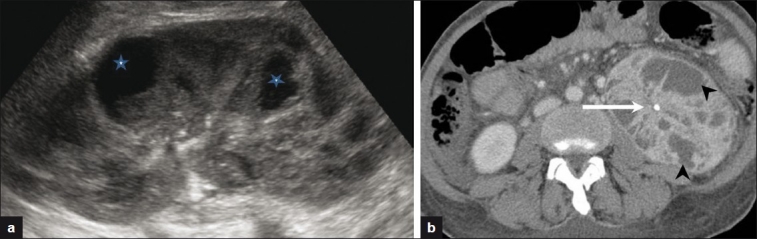
Background: Xanthogranulomatous pyelonephritis (XGN) is an uncommon condition characterized by chronic suppurative renal inflammation that leads to progressive parenchymal destruction.
Purpose: To review the computed tomography (CT) findings of patients diagnosed with XGN.
Materials and methods: A retrospective review of CT findings in patients with histologically proven XGN was carried out.
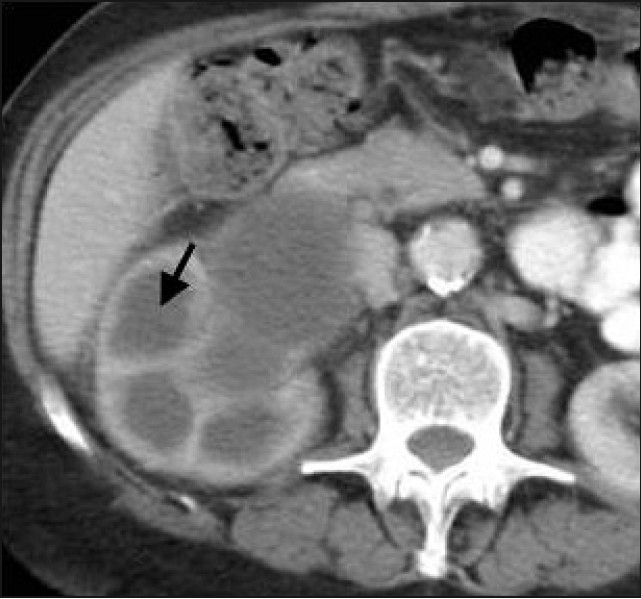
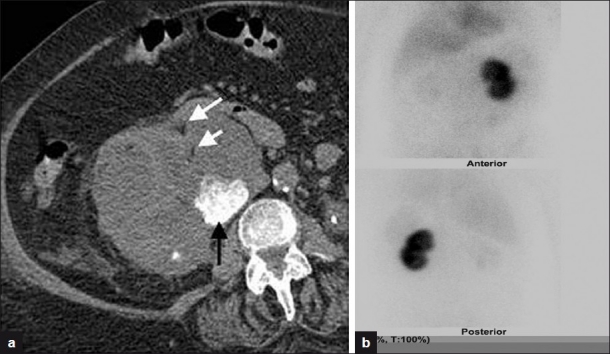
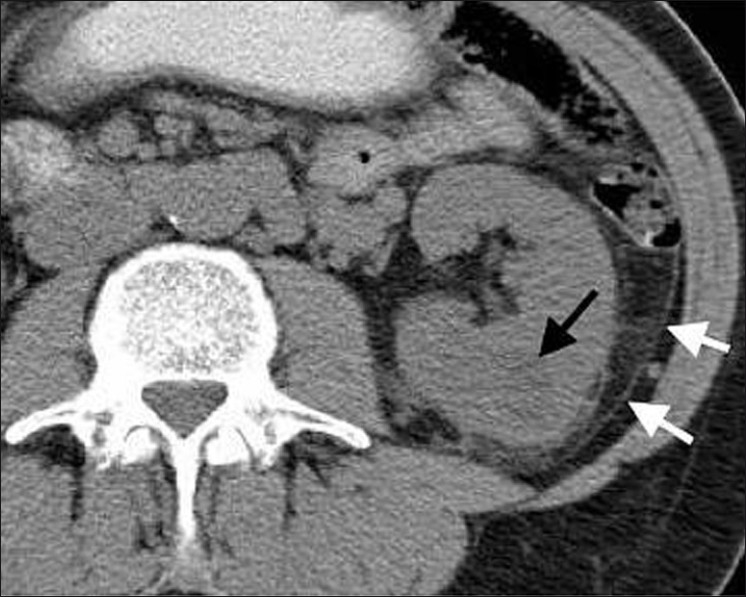
Results: Thirteen CT examinations of 11 patients were analyzed. Renal enlargement was demonstrable on the affected side in all patients. Nine patients (82%) had multiple dilated calyces and abnormal parenchyma. Six patients (55%) had a renal pelvis or upper ureteric calculus causing obstruction. Three patients (27%) had focal fat deposits identifiable within the inflamed renal parenchyma. Two patients had renal abscesses. Ten patients (91%) had extrarenal extension of the inflammatory changes. Three patients (27%) demonstrated extensive retroperitoneal inflammation.
Conclusion: Unilateral renal enlargement and inflammation were the most consistent findings of XGN on CT. Perinephric inflammation and collections or abscess should also alert the radiologist to the possibility of this diagnosis.
Keywords: Xanthogranulomatous pyelonephritis; computed tomography; perinephric inflammation.
Conflict of interest statement
Figures

References
-
- Kumar V, Abbas A, Fausto N, editors. Robbins and Cotran Pathologic Basis of Disease. 7th ed. Philadelphia, Pa: Saunders Elsevier; 2005.
-
- Hayes WS, Hartman DS, Sesterbenn IA. Xanthogranulomatous pyelonephritis. Radiographics. 1991;11:485–98. - PubMed
-
- Clapton WK, Boucaut HA, Dewan PA, Bourne AJ, Byard RW. Clinicopathological features of xanthogranulomatous pyelonephritis in infancy. Pathology. 1993;25:110–3. - PubMed
-
- Fan CM, Whitman GJ, Chew FS. Xanthogranulomatous pyelonephritis. AJR Am J Roentgenol. 1995;165:1008. - PubMed
-
- Dwivedi US, Goyal NK, Saxena V, Acharya RL, Trivedi S, Singh PB, et al. Xanthogranulomatous pyelonephritis: Our experience with review of published reports. ANZ J Surg. 2006;76:1007–9. - PubMed
LinkOut - more resources
Full Text Sources