

FRAX or fiction: determining optimal screening strategies for treatment of osteoporosis in residents in long-term care facilities
- PMID: 22316237
- PMCID: PMC3477847
- DOI: 10.1111/j.1532-5415.2011.03884.x
FRAX or fiction: determining optimal screening strategies for treatment of osteoporosis in residents in long-term care facilities
Abstract
Objectives: To examine screening strategies for osteoporosis and fractures for treatment of long-term care residents.
Design: Cross-sectional analysis to examine screening strategies for treatment.
Setting: Assisted living and skilled care facilities.
Participants: Two hundred two frail women aged 65 and older (mean 85), excluding those receiving bisphosphonates.
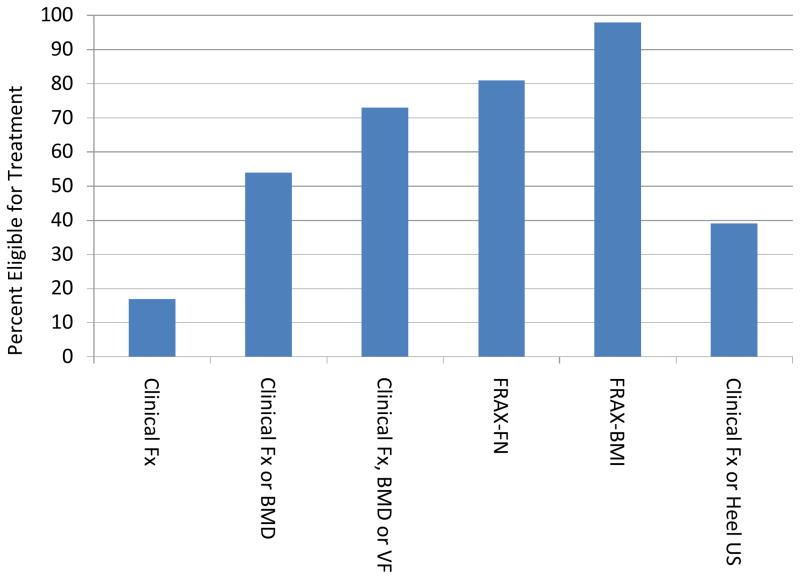
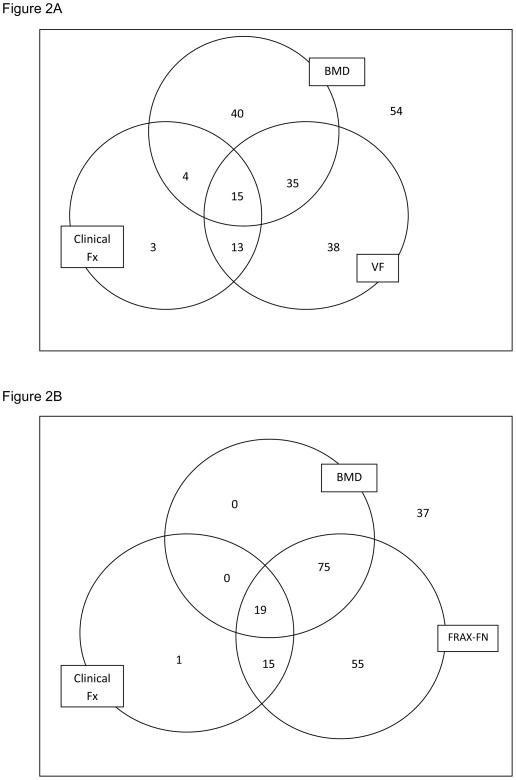
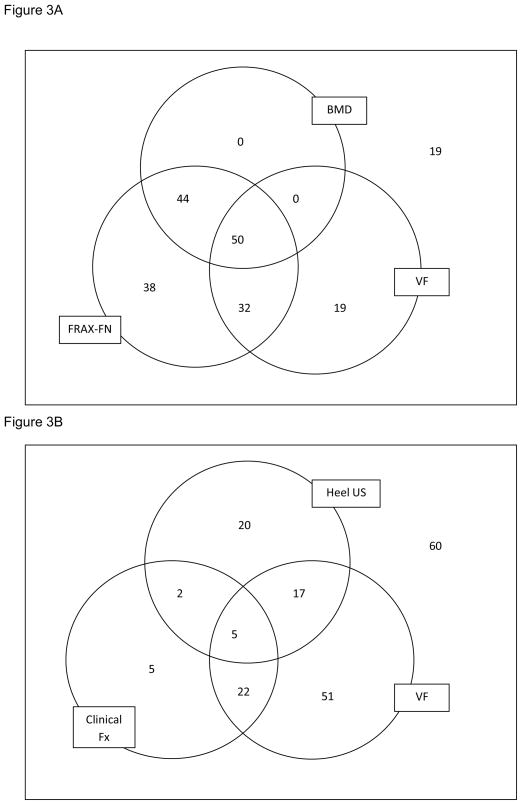
Measurements: Clinical fractures of the hip or spine (Clin Fx); Clin Fx or bone mineral density (BMD); Clin Fx, BMD, or vertebral fractures (VF) assessed according to dual-energy X-ray absorptiometry-based vertebral fracture assessments; fracture risk algorithm using femoral neck BMD (FRAX-FN); fracture risk algorithm using body mass index (FRAX-BMI); or Clin Fx or heel ultrasound (heel US).
Results: Treatment eligibility ranged from 17% (Clin Fx) to 98% (FRAX-BMI). VFs were found in 47%, 74% of which were silent. Criteria with Clin Fx, BMD, or VF identified 73% of study participants for treatment. FRAX-FN suggested treatment in 81% but would have missed approximately 10% of individuals with silent VFs. Clin Fx or heel US suggested that 39% of participants were eligible for treatment.
Conclusion: Long-term care residents eligible for osteoporosis treatment ranged from fewer than 20% to roughly all residents depending on screening criteria. VFs are common and identify a subset of residents missed by conventional BMD scans or FRAX-FN. A reasonable clinical approach could consider treatment for those with Clin Fx of the hip or spine, radiological evidence of a VF, or osteoporosis according to BMD classification. Prospective studies are needed to determine optimal screening strategies for treatment in this cohort.
© 2012, Copyright the Authors Journal compilation © 2012, The American Geriatrics Society.
Conflict of interest statement
Figures
Comment in
-
Screening strategies for treatment of osteoporosis in long-term care residents.J Am Geriatr Soc. 2012 Dec;60(12):2383-4; author reply 2384. doi: 10.1111/jgs.12024. J Am Geriatr Soc. 2012. PMID: 23231569 No abstract available.
References
-
- Cummings SR, Kelsey JL, Nevitt MC, et al. Epidemiology of osteoporosis and osteoporotic fractures. Epidemiol Rev. 1985;7:178–208. - PubMed
-
- Cummings SR. Should perimenopausal women be screened for osteoporosis? Ann Intern Med. 1986;104:817–23. - PubMed
-
- Melton LJ, III, O’Fallon WM, Riggs BL. Secular trends in the incidence of hip fractures. Calcif Tissue Int. 1987;41:57–64. - PubMed
-
- Kelsey JL, Hoffman S. Risk factors for hip fracture. N Engl J Med. 1987;316:404–406. - PubMed
-
- Zimmerman SI, Girman CJ, Buie VC, et al. The prevalence of osteoporosis in nursing home residents. Osteoporos Int. 1999;9:151–157. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
