

Stroke With Transfusions Changing to Hydroxyurea (SWiTCH)
- PMID: 22318199
- PMCID: PMC3350359
- DOI: 10.1182/blood-2011-11-392340
Stroke With Transfusions Changing to Hydroxyurea (SWiTCH)
Abstract
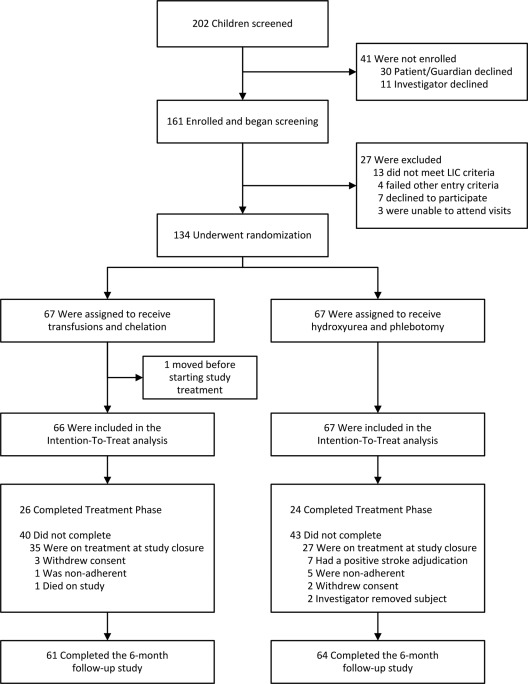
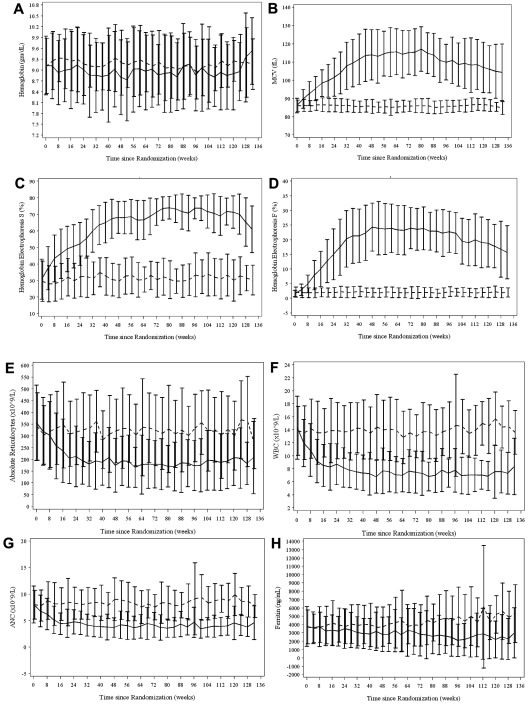
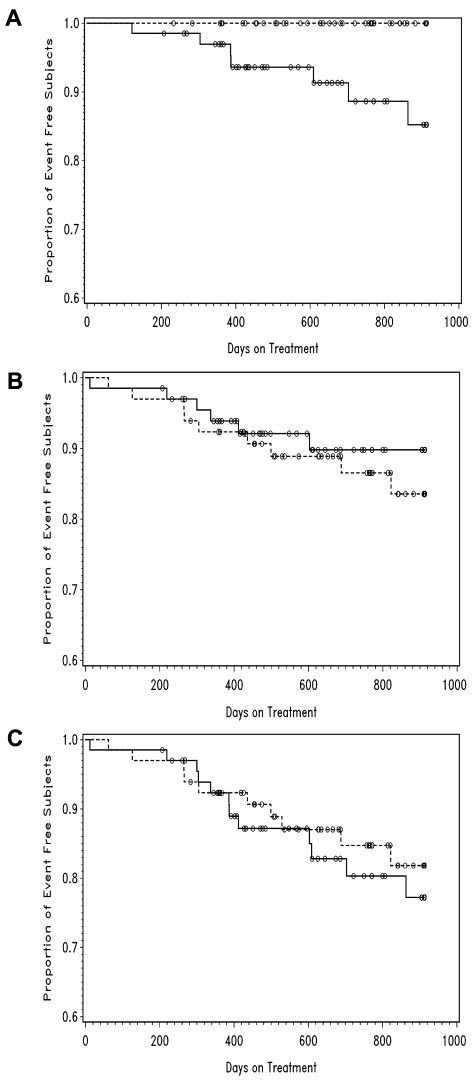
Stroke is a devastating complication of sickle cell anemia (SCA) with high recurrence if untreated. Chronic transfusions reduce recurrent strokes but have associated morbidities including iron overload. Stroke With Transfusions Changing to Hydroxyurea (SWiTCH) was a multicenter phase 3 randomized trial comparing standard treatment (transfusions/chelation) to alternative treatment (hydroxyurea/phlebotomy) for children with SCA, stroke, and iron overload. SWiTCH was a noninferiority trial with a composite primary end point, allowing an increased stroke risk but requiring superiority for removing iron. Subjects on standard treatment received monthly transfusions plus daily deferasirox iron chelation. Subjects on alternative treatment received hydroxyurea plus overlap transfusions during dose escalation to maximum tolerated dose (MTD), followed by monthly phlebotomy. Subjects on standard treatment (N = 66) maintained 30% sickle hemoglobin (HbS) and tolerated deferasirox at 28.2 ± 6.0 mg/kg/d. Subjects on alternative treatment (N = 67) initiated hydroxyurea and 60 (90%) reached MTD at 26.2 ± 4.9 mg/kg/d with 29.1% ± 6.7% fetal hemoglobin (HbF). Adjudication documented no strokes on transfusions/chelation but 7 (10%) on hydroxyurea/phlebotomy, still within the noninferiority stroke margin. The National Heart, Lung, and Blood Institute closed SWiTCH after interim analysis revealed equivalent liver iron content, indicating futility for the composite primary end point. Transfusions and chelation remain a better way to manage children with SCA, stroke, and iron overload.
Trial registration: ClinicalTrials.gov NCT00122980.
Figures
Comment in
-
To SWiTCH or not to SWiTCH?Blood. 2012 Apr 26;119(17):3870-1. doi: 10.1182/blood-2012-02-410951. Blood. 2012. PMID: 22538492
References
-
- Ohene-Frempong K. Stroke in sickle cell disease: demographic, clinical, and therapeutic considerations. Semin Hematol. 1991;28(3):213–219. - PubMed
-
- Powars D, Wilson B, Imbus C, Pegelow C, Allen J. The natural history of stroke in sickle cell disease. Am J Med. 1978;65(3):461–471. - PubMed
-
- Ohene-Frempong K, Weiner SJ, Sleeper LA, et al. Cerebrovascular accidents in sickle cell disease: rates and risk factors. Blood. 1998;91(1):288–294. - PubMed
-
- Balkaran B, Char G, Morris JS, et al. Stroke in a cohort of patients with homozygous sickle cell disease. J Pediatr. 1992;120(3):360–366. - PubMed
-
- Moohr JW, Wilson H, Pang EJ-M. Strokes and their management in sickle cell disease. In: Fried W, editor. Comparative Clinical Aspects of Sickle Cell Disease. Amsterdam, The Netherlands: Elsevier North Holland; 1982. pp. 101–111.
