

Influence of the National Trauma Data Bank on the study of trauma outcomes: is it time to set research best practices to further enhance its impact?
- PMID: 22321521
- PMCID: PMC3334459
- DOI: 10.1016/j.jamcollsurg.2011.12.013
Influence of the National Trauma Data Bank on the study of trauma outcomes: is it time to set research best practices to further enhance its impact?
Abstract
Background: Risk-adjusted analyses are critical in evaluating trauma outcomes. The National Trauma Data Bank (NTDB) is a statistically robust registry that allows such analyses; however, analytical techniques are not yet standardized. In this study, we examined peer-reviewed manuscripts published using NTDB data, with particular attention to characteristics strongly associated with trauma outcomes. Our objective was to determine if there are substantial variations in the methodology and quality of risk-adjusted analyses and therefore, whether development of best practices for risk-adjusted analyses is warranted.
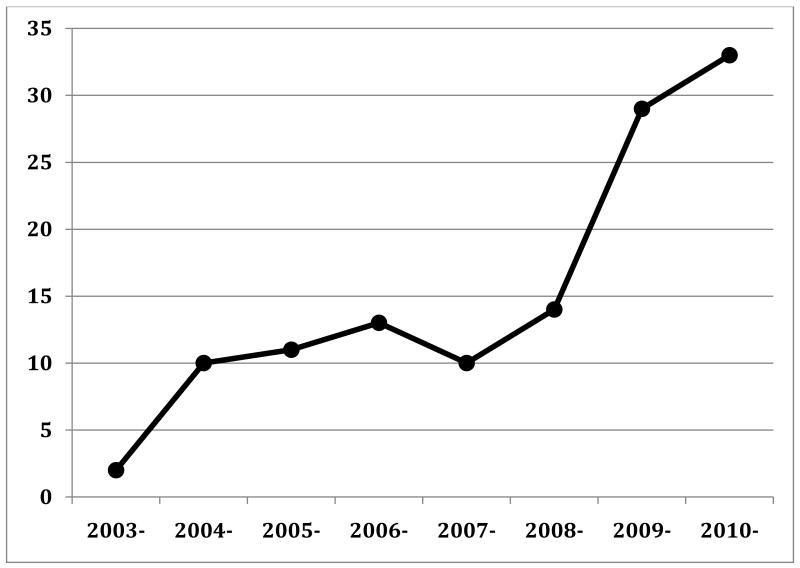
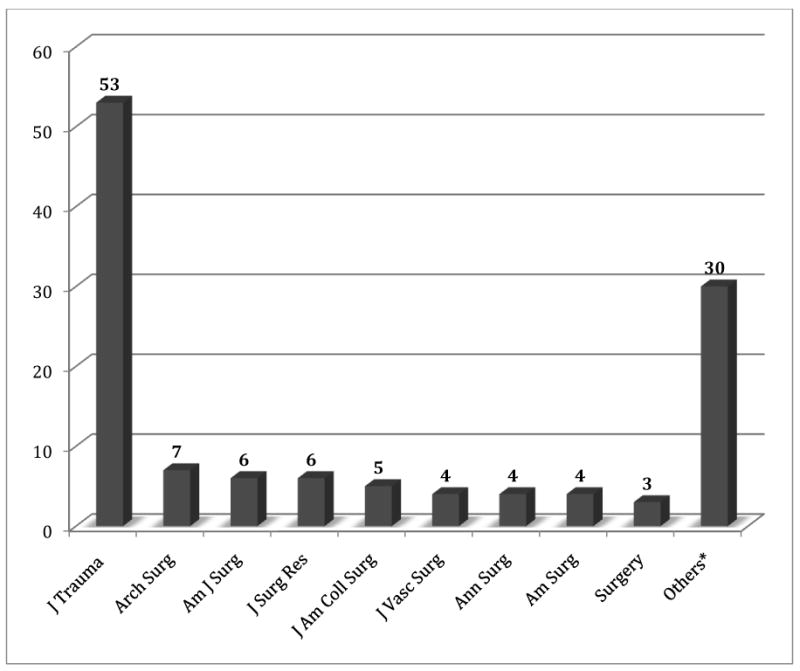
Study design: A database of all studies using NTDB data published through December 2010 was created by searching PubMed and Embase. Studies with multivariate risk-adjusted analyses were examined for their central question, main outcomes measures, analytical techniques, covariates in adjusted analyses, and handling of missing data.
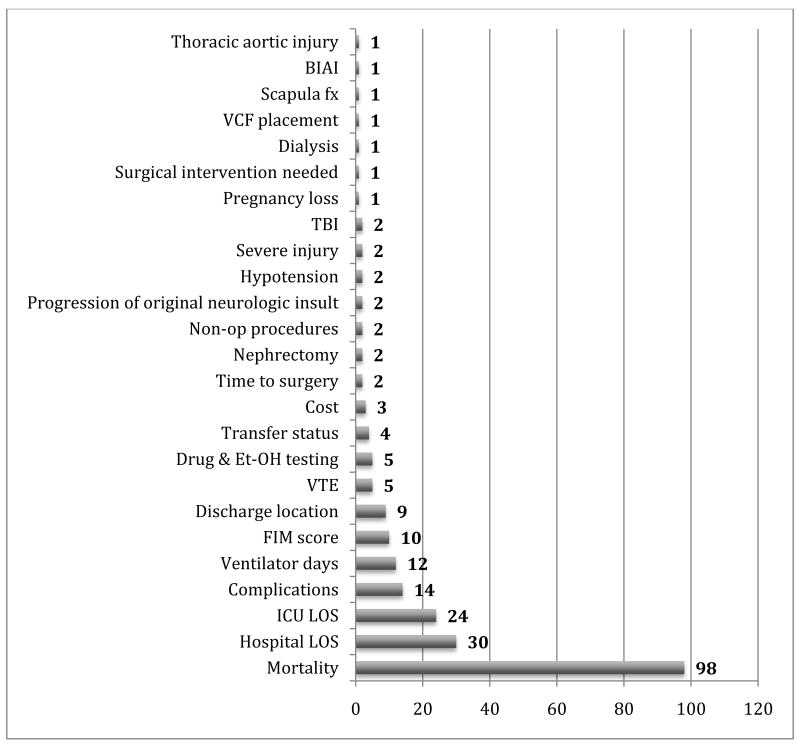
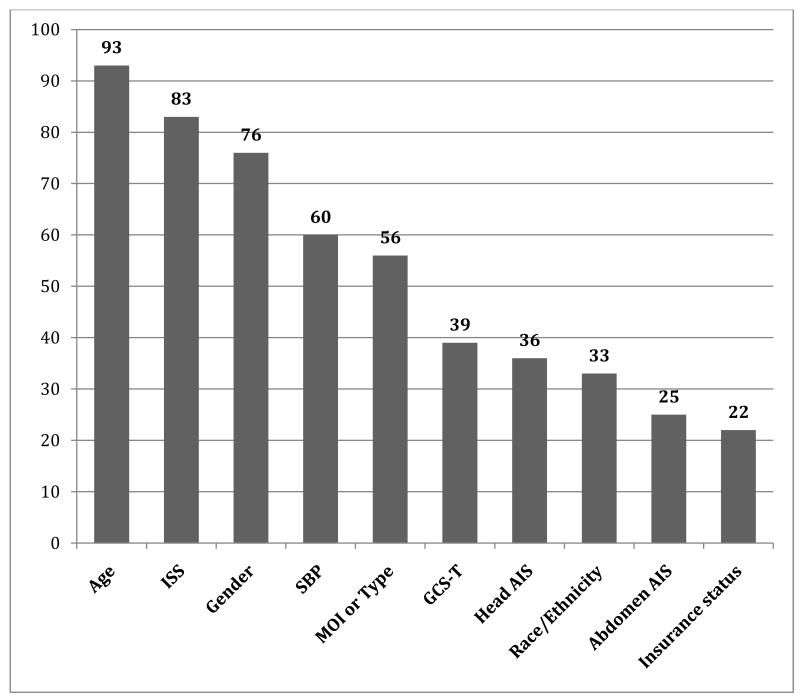
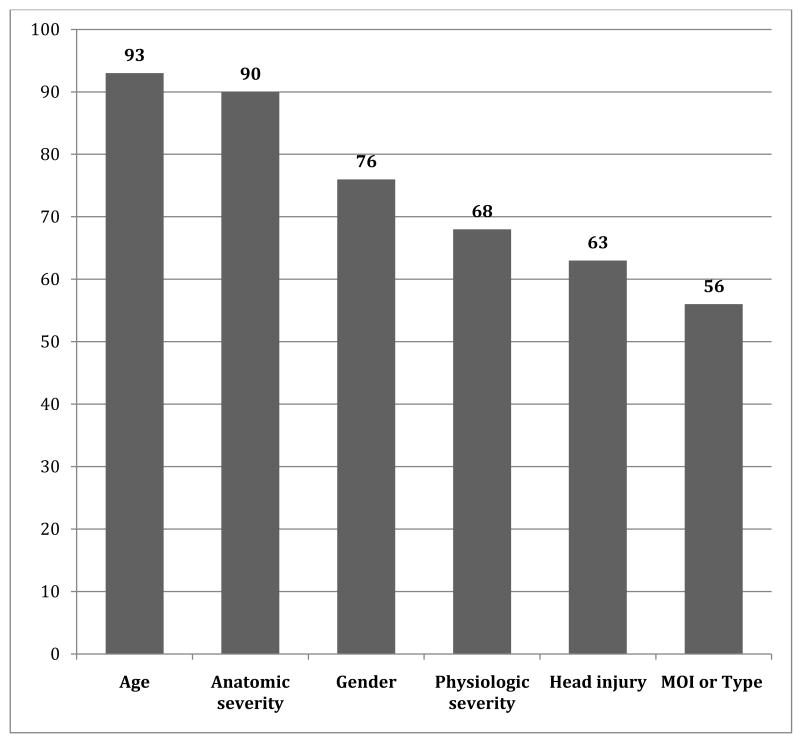
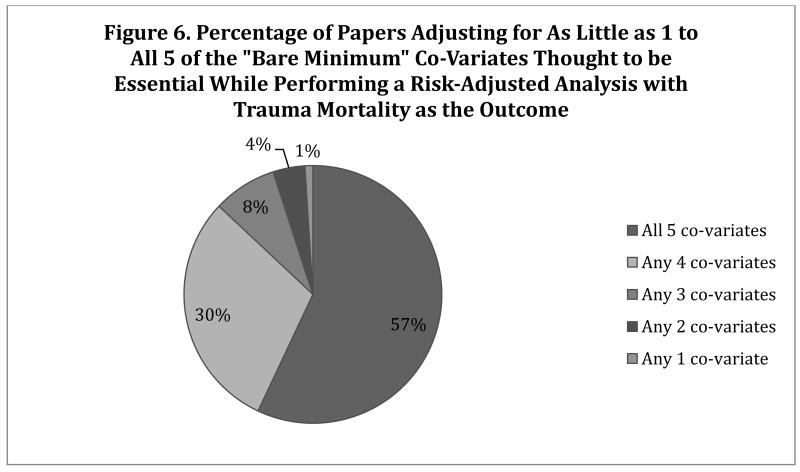
Results: Of 286 NTDB publications, 122 performed a multivariable adjusted analysis. These studies focused on clinical outcomes (51 studies), public health policy or injury prevention (30), quality (16), disparities (15), trauma center designation (6), or scoring systems (4). Mortality was the main outcome in 98 of these studies. There were considerable differences in the covariates used for case adjustment. The 3 covariates most frequently controlled for were age (95%), Injury Severity Score (85%), and sex (78%). Up to 43% of studies did not control for the 5 basic covariates necessary to conduct a risk-adjusted analysis of trauma mortality. Less than 10% of studies used clustering to adjust for facility differences or imputation to handle missing data.
Conclusions: There is significant variability in how risk-adjusted analyses using data from the NTDB are performed. Best practices are needed to further improve the quality of research from the NTDB.
Copyright © 2012 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Center for Disease Control and Prevention (CDC) Injury Control Homepage. [Accessed on May 12, 2011]; Available at: http://www.cdc.gov/injury/
-
- NCHS. National health statistics reports, no 29. Atlanta, GA: 2010. National hospital discharge survey: 2007 summary. - PubMed
-
- Finkelstein EA, Corso PS, Miller TR Associates. Incidence and economic burden of injuries in the United States. New York, NY: Oxford University Press; 2006.
-
- National Trauma Data Standard Data Dictionary 2011 Admissions. [Accessed on May 12, 2011]; Available at: http://www.ntdsdictionary.org/dataElements/documents/NTDS2011_Final3.pdf.
-
- Roudsari B, Field C, Caetano R. Clustered and missing data in the US National Trauma Data Bank: implications for analysis. Inj Prev. 2008;14:96–100. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
