

Maternal pre-pregnancy weight and gestational weight gain and their association with birthweight with a focus on racial differences
- PMID: 22322428
- PMCID: PMC3677820
- DOI: 10.1007/s10995-012-0950-x
Maternal pre-pregnancy weight and gestational weight gain and their association with birthweight with a focus on racial differences
Abstract
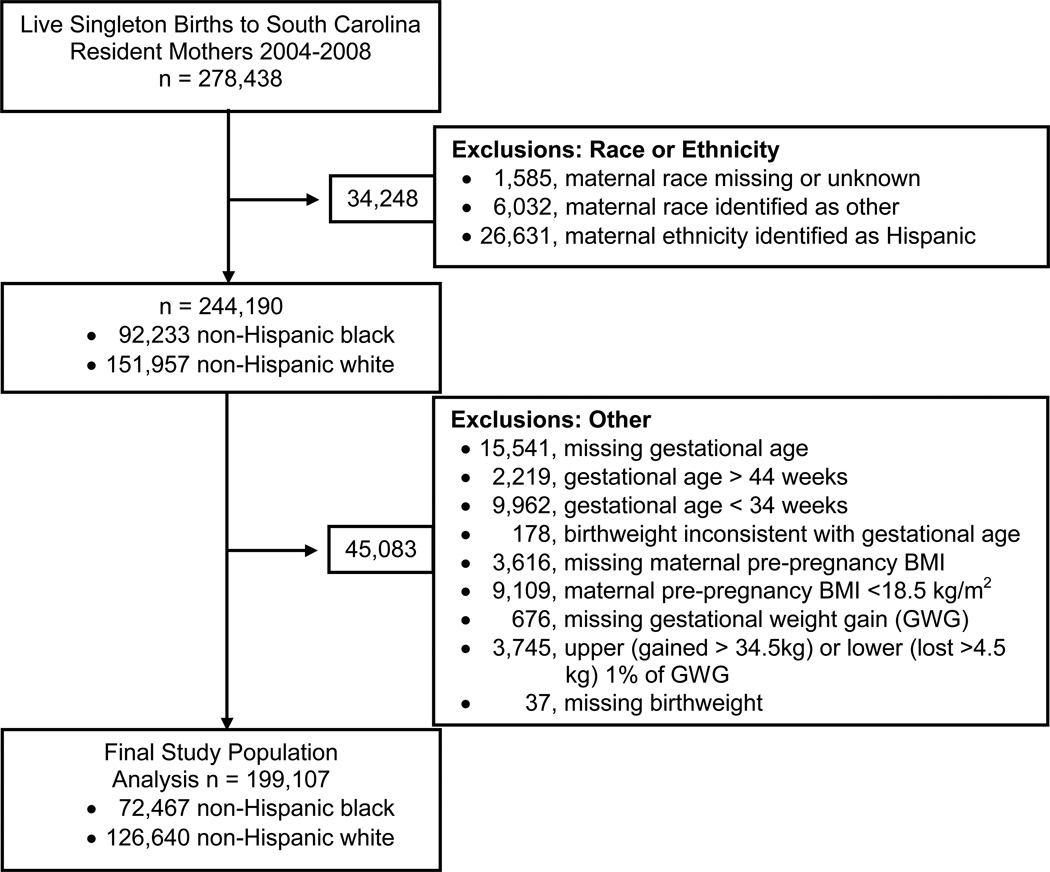
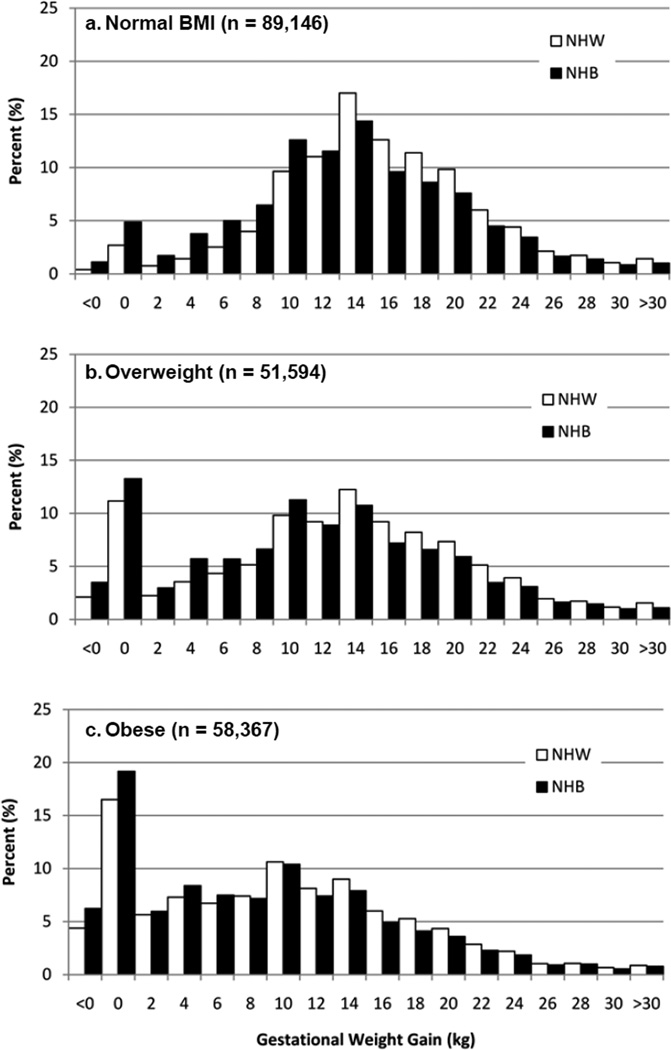
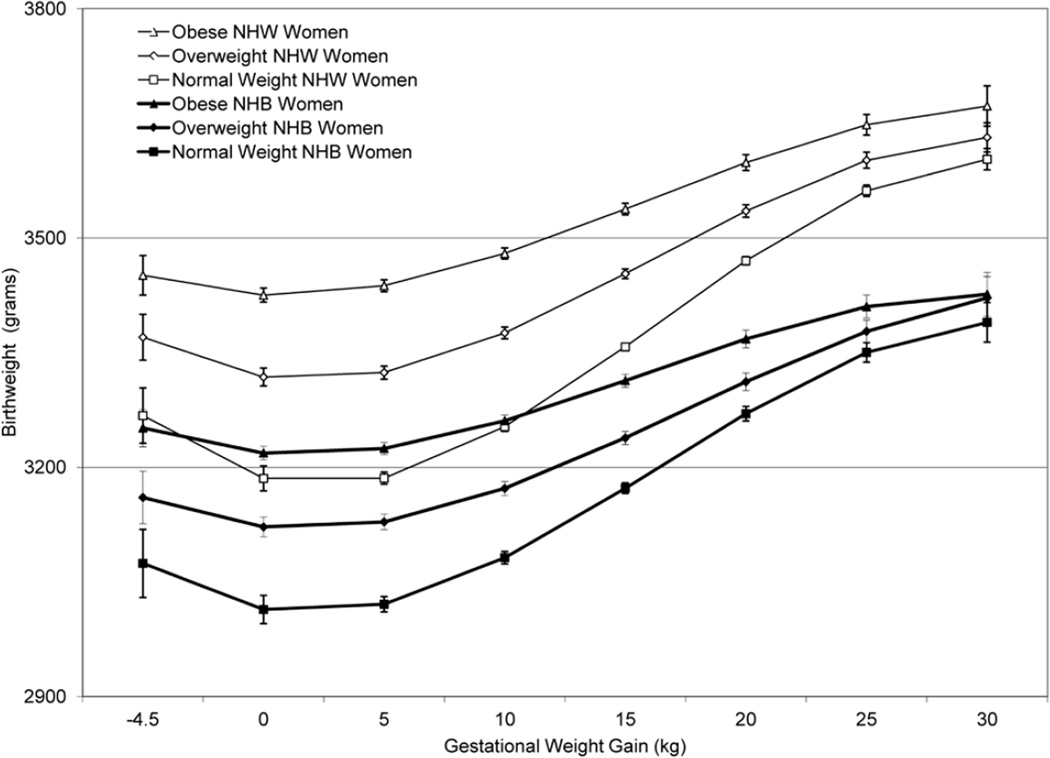
Our objectives were to examine the interaction between maternal pre-pregnancy body mass index (BMI) and gestational weight gain (GWG) and their association with birthweight, with a focus on racial differences. We used birth certificate data from live singleton births of South Carolina resident mothers, who self-reported their race as non-Hispanic white (NHW, n = 140, 128) or non-Hispanic black (NHB, n = 82,492) and who delivered at 34-44 weeks of gestation between 2004 and 2008 to conduct a cross-sectional study. Linear regression was used to examine the relationship between our exposures (i.e., race, BMI and GWG) and our outcome birthweight. Based on 2009 Institute of Medicine guidelines, the prevalence of adequate, inadequate and excessive GWG was 27.1, 24.2 and 48.7%, respectively, in NHW women and 24.2, 34.8 and 41.0%, respectively, in NHB women. Adjusting for infant sex, gestational age, maternal age, tobacco use, education, prenatal care, and Medicaid, the difference in birthweight between excessive and adequate GWG at a maternal BMI of 30 kg/m(2) was 118 g (95% CI: 109, 127) in NHW women and 101 g (95% CI: 91, 111) in NHB women. Moreover, excessive versus adequate GWG conveyed similar protection from having a small for gestational age infant in NHW [OR = 0.64 (95% CI 0.61, 0.67)] and NHB women [OR = 0.68 (95% CI: 0.65, 0.72)]. In conclusion, we report a strong association between excessive GWG and higher infant birthweight across maternal BMI classes in NHW and NHB women. Given the high prevalence of excessive GWG even a small increase in birthweight may have considerable implications at the population level.
Conflict of interest statement
Figures

References
-
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults: 1999–2008. JAMA. 2010;303:235–241. - PubMed
-
- Institute of Medicine and National Research Council 2009. Weight gain during pregnancy: reexamining the guidelines. Washington, DC: The national Academies Press; 2011. - PubMed
-
- Siega-Riz AM, Viswanathan M, Moos MK, Deierlein A, Mumford S, Knaack J, Thieda P, Lux LJ, Lohr KN. A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: birthweight, fetal growth, and postpartum weight retention. Am.J.Obstet.Gynecol. 2009;201:339–314. - PubMed
-
- Alexander GR, Tompkins ME, Allen MC, Hulsey TC. Trends and racial differences in birth weight and related survival. Matern.Child Health J. 1999;3:71–79. - PubMed
-
- Alexander GR, Wingate MS, Bader D, Kogan MD. The increasing racial disparity in infant mortality rates: composition and contributors to recent US trends. Am.J Obstet.Gynecol. 2007 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
