

Excimer laser smoothing of endothelial keratoplasty grafts
- PMID: 22322485
- PMCID: PMC3299824
- DOI: 10.1097/ICO.0b013e31822444a7
Excimer laser smoothing of endothelial keratoplasty grafts
Abstract
Purpose: To use excimer laser smoothing passes to reshape Descemet-stripping automated endothelial keratoplasty (DSAEK) endothelial grafts and to evaluate the effect on the donor endothelium.
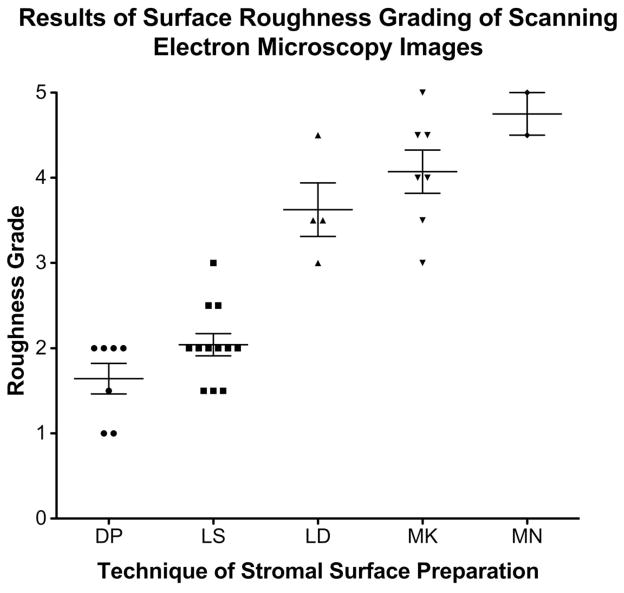
Methods: The stromal surface of microkeratome-cut DSAEK grafts was smoothed using excimer laser smoothing passes with masking fluid. Excimer laser hyperopic ablation was used to improve the uniformity of graft thickness within the optical zone. Fourier-domain optical coherence tomography was used to measure endothelial graft pachymetry, plan ablations, and evaluate donor contour. Vital dye staining was performed to assess endothelial cell damage. Scanning electron microscopy images of stromal surfaces were graded on a 5-point scale by masked observers to evaluate surface roughness.
Results: Four grafts underwent excimer laser smoothing. Vital dye staining showed no endothelial damage. Microkeratome-cut surfaces treated with laser smoothing (mean grade = 2.04) were smoother than nonsmoothed microkeratome-cut surfaces (mean grade = 4.07; P < 0.01), surfaces that underwent dry laser ablation (mean grade = 3.63; P < 0.01) and manually dissected interfaces (mean grade = 4.75; P < 0.0001). No difference was observed between stromal beds created by peeling Descemet membrane (mean grade = 1.64) compared with surfaces produced by microkeratome cutting followed by laser smoothing (mean grade = 2.04; P = 0.14). One graft underwent combined excimer smoothing and peripheral hyperopic ablation. The center-periphery thickness difference was 15 μm before ablation and 4 μm afterward.
Conclusions: Laser smoothing passes can be used to improve the contour and smoothness of DSAEK grafts without damaging donor endothelial cells. Clinical trials are needed to determine whether reshaping donors using excimer laser can deliver improved visual outcomes after DSAEK.
Figures





Similar articles
-
Deep Laser-Assisted Lamellar Anterior Keratoplasty With Microkeratome-Cut Grafts.Cornea. 2016 May;35(5):706-12. doi: 10.1097/ICO.0000000000000783. Cornea. 2016. PMID: 26890667 Free PMC article.
-
Dual laser-assisted lamellar anterior keratoplasty with top hat graft: a laboratory study.Cornea. 2012 Jul;31(7):791-7. doi: 10.1097/ICO.0b013e318226da35. Cornea. 2012. PMID: 22378114 Free PMC article.
-
Visual outcome and histological findings following femtosecond laser-assisted versus microkeratome-assisted DSAEK.Graefes Arch Clin Exp Ophthalmol. 2013 Aug;251(8):1979-85. doi: 10.1007/s00417-013-2359-7. Epub 2013 May 10. Graefes Arch Clin Exp Ophthalmol. 2013. PMID: 23661098
-
[Corneal power after descemet stripping automated endothelial keratoplasty (DSAEK) - Modeling and concept for calculation of intraocular lenses].Z Med Phys. 2016 Jun;26(2):120-6. doi: 10.1016/j.zemedi.2015.02.003. Epub 2015 Mar 17. Z Med Phys. 2016. PMID: 25791739 Review. German.
-
Ultrathin Descemet stripping automated endothelial keratoplasty.Curr Opin Ophthalmol. 2019 Jul;30(4):264-270. doi: 10.1097/ICU.0000000000000575. Curr Opin Ophthalmol. 2019. PMID: 31033735 Review.
Cited by
-
Deep Laser-Assisted Lamellar Anterior Keratoplasty With Microkeratome-Cut Grafts.Cornea. 2016 May;35(5):706-12. doi: 10.1097/ICO.0000000000000783. Cornea. 2016. PMID: 26890667 Free PMC article.
-
Eye-bank preparation of endothelial tissue.Curr Opin Ophthalmol. 2014 Jul;25(4):319-24. doi: 10.1097/ICU.0000000000000060. Curr Opin Ophthalmol. 2014. PMID: 24837574 Free PMC article. Review.
References
-
- Price MO, Price FW., Jr Descemet’s stripping with endothelial keratoplasty: comparative outcomes with microkeratome-dissected and manually dissected donor tissue. Ophthalmology. 2006 Nov;113(11):1936–1942. - PubMed
-
- Chen ES, Terry MA, Shamie N, Hoar KL, Friend DJ. Descemet-stripping automated endothelial keratoplasty: six-month results in a prospective study of 100 eyes. Cornea. 2008 Jun;27(5):514–520. - PubMed
-
- Chen ES, Terry MA, Shamie N, Hoar KL, Phillips PM, Friend DJ. Endothelial keratoplasty: vision, endothelial survival, and complications in a comparative case series of fellows vs attending surgeons. Am J Ophthalmol. 2009 Jul;148(1):26–31. e22. - PubMed
-
- Bahar I, Kaiserman I, Levinger E, Sansanayudh W, Slomovic AR, Rootman DS. Retrospective contralateral study comparing descemet stripping automated endothelial keratoplasty with penetrating keratoplasty. Cornea. 2009 Jun;28(5):485–488. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
