

Spurious inferences about long-term outcomes: the case of severe sepsis and geriatric conditions
- PMID: 22323301
- PMCID: PMC3360570
- DOI: 10.1164/rccm.201109-1660OC
Spurious inferences about long-term outcomes: the case of severe sepsis and geriatric conditions
Abstract
Rationale: Survivors of critical illness suffer significant limitations and disabilities.
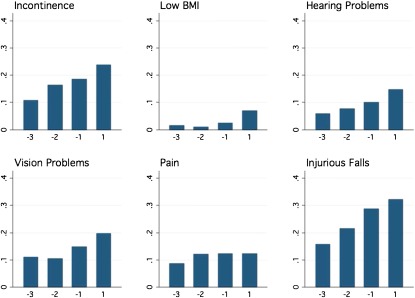
Objectives: Ascertain whether severe sepsis is associated with increased risk of so-called geriatric conditions (injurious falls, low body mass index [BMI], incontinence, vision loss, hearing loss, and chronic pain) and whether this association is measured consistently across three different study designs.
Methods: Patients with severe sepsis were identified in the Health and Retirement Study, a nationally representative cohort interviewed every 2 years, 1998 to 2006, and in linked Medicare claims. Three comparators were used to assess an association of severe sepsis with geriatric conditions in survivors: the prevalence in the United States population aged 65 years and older, survivors' own pre-sepsis levels assessed before hospitalization, or survivors' own pre-sepsis trajectory.
Measurements and main results: Six hundred twenty-three severe sepsis hospitalizations were followed a median of 0.92 years. When compared with the 65 years and older population, surviving severe sepsis was associated with increased rates of low BMI, injurious falls, incontinence, and vision loss. Results were similar when comparing survivors to their own pre-sepsis levels. The association of low BMI and severe sepsis persisted when controlling for patients' pre-sepsis trajectories, but there was no association of severe sepsis with injurious falls, incontinence, vision loss, hearing loss, and chronic pain after such controls.
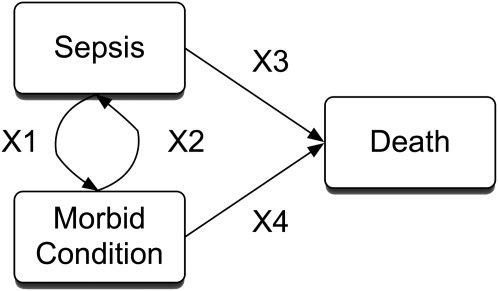
Conclusions: Geriatric conditions are common after severe sepsis. However, severe sepsis is associated with increased rates of only a subset of geriatric conditions, not all. In studying outcomes after acute illness, failing to measure and control for both preillness levels and trajectories may result in erroneous conclusions.
Figures
Comment in
-
Does the hospital make you older faster?Am J Respir Crit Care Med. 2012 Apr 15;185(8):796-8. doi: 10.1164/rccm.201202-0267ED. Am J Respir Crit Care Med. 2012. PMID: 22505749 No abstract available.
-
Fatalism is not justified when evaluating the critically ill elderly.Am J Respir Crit Care Med. 2012 Aug 1;186(3):290; author reply 290-1. doi: 10.1164/ajrccm.186.3.290. Am J Respir Crit Care Med. 2012. PMID: 22855544 Free PMC article. No abstract available.
References
-
- Desai SV, Law TJ, Needham DM. Long-term complications of critical care. Crit Care Med 2011;39:371–379 - PubMed
-
- Cheung AM, Tansey CM, Tomlinson G, Diaz-Granados N, Matte A, Barr A, Mehta S, Mazer CD, Guest CB, Stewart TE, et al. Two-year outcomes, health care use, and costs of survivors of acute respiratory distress syndrome. Am J Respir Crit Care Med 2006;174:538–544 - PubMed
-
- Dowdy DW, Eid MP, Dennison CR, Mendez-Tellez PA, Herridge MS, Guallar E, Pronovost PJ, Needham DM. Quality of life after acute respiratory distress syndrome: a meta-analysis. Intensive Care Med 2006;32:1115–1124 - PubMed
-
- Granja C, Morujao E, Costa-Pereira A. Quality of life in acute respiratory distress syndrome survivors may be no worst than in other ICU survivors. Intensive Care Med 2003;29:1744–1750 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
