Impact of changing trends in medical therapy on surgery for benign prostatic hyperplasia over two decades
- PMID: 22323970
- PMCID: PMC3272552
- DOI: 10.4111/kju.2012.53.1.23
Impact of changing trends in medical therapy on surgery for benign prostatic hyperplasia over two decades
Abstract
Purpose: Following the introduction of medical therapy for benign prostatic hyperplasia (BPH), we determined the effect of the change in trends in medical therapy on the indication and outcome of surgical intervention for BPH.
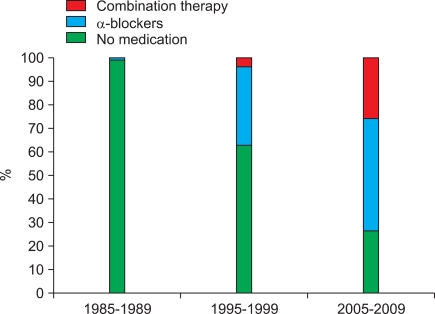
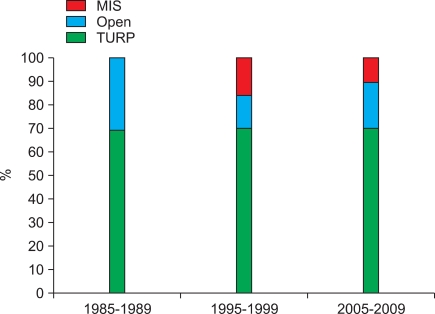
Materials and methods: We compared the basic characteristics of, weight of resected tissue of, transfusions in, and postoperative complications of patients who underwent surgery between 1985 and 1989 (before the advent of medical therapy for BPH), between 1995 and 1999 (when medical therapy was developed and became widely used as alternative treatment), and between 2005 and 2009 (when medical therapy superseded surgical intervention to become first-line treatment and when combination therapy became widely adopted).
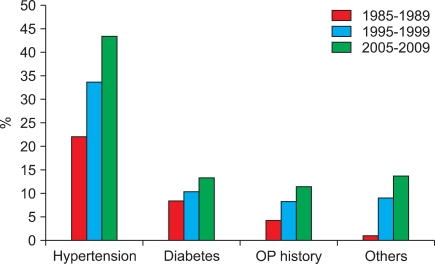
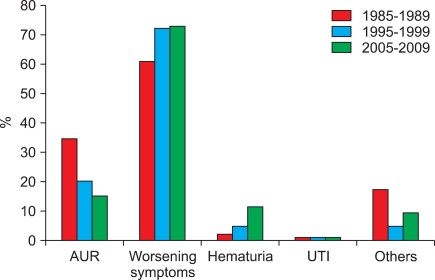
Results: At our institution, the mean age and BMI of patients increased over the past two decades (p<0.001). Hypertension, operation history, and other comorbidities also increased significantly (p<0.001, p=0.005, and p<0.001, respectively). The indications for surgery in 1985 to 1989, 1995 to 1999, and 2005 to 2009 were as follows: acute urinary retention in 34.7%, 20.2%, and 15.1% of patients and symptomatic deterioration in 61.1%, 72.3%, and 73.0% of patients, respectively. Prostate volume and the weight of resected tissue increased from 34.4±14.5 ml to 61.3±32.4 ml and from 7.2±6.4 g to 10.8±7.6 g, respectively, over two decades. Patients who underwent surgery in 2005 to 2009 had their catheters removed earlier (p<0.001). Secondary hemorrhage within four postoperative weeks and repeat transurethral resection of the prostate within 1 year decreased significantly (p=0.03 and p=0.003, respectively). No statistically significant change in impaired detrusor contractility was found (p=0.523).
Conclusions: Although patients who underwent surgery were older after widespread use of medical therapy for BPH, advancements in surgical techniques have benefitted these patients.
Keywords: Benign prostatic hyperplasia; Medical therapy; Surgical intervention.
Conflict of interest statement
The authors have nothing to disclose.
Figures
References
-
- Flanigan RC, Reda DJ, Wasson JH, Anderson RJ, Abdellatif M, Bruskewitz RC. 5-year outcome of surgical resection and watchful waiting for men with moderately symptomatic benign prostatic hyperplasia: a Department of Veterans Affairs cooperative study. J Urol. 1998;160:12–16. - PubMed
-
- Reich O, Gratzke C, Stief CG. Techniques and long-term results of surgical procedures for BPH. Eur Urol. 2006;49:970–978. - PubMed
-
- Chung BH, Yang KM, Hong SJ. Meta-analysis of alpha receptor antagosist for benign prostatic hyperplasia from papers that were published in Korea. Korean J Urol. 2005;46:252–258.
-
- Lepor H, Auerbach S, Puras-Baez A, Narayan P, Soloway M, Lowe F, et al. A randomized, placebo-controlled multicenter study of the efficacy and safety of terazosin in the treatment of benign prostatic hyperplasia. J Urol. 1992;148:1467–1474. - PubMed
-
- McConnell JD, Roehrborn CG, Bautista OM, Andriole GL, Jr, Dixon CM, Kusek JW, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349:2387–2398. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous