

Myeloablative transplantation using either cord blood or bone marrow leads to immune recovery, high long-term donor chimerism and excellent survival in chronic granulomatous disease
- PMID: 22326631
- PMCID: PMC3540103
- DOI: 10.1016/j.bbmt.2012.02.002
Myeloablative transplantation using either cord blood or bone marrow leads to immune recovery, high long-term donor chimerism and excellent survival in chronic granulomatous disease
Abstract
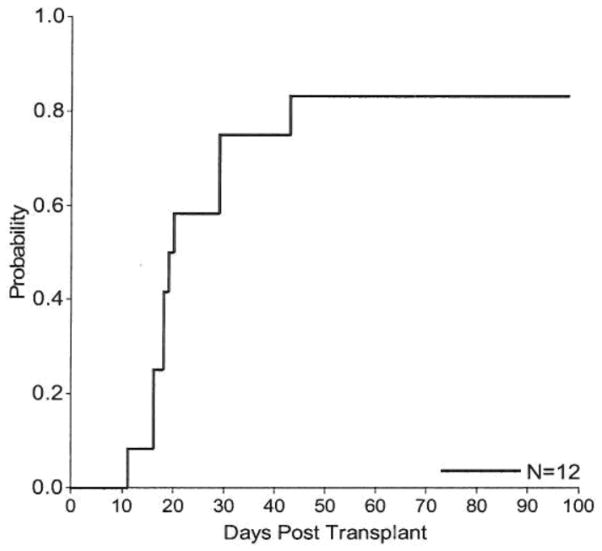
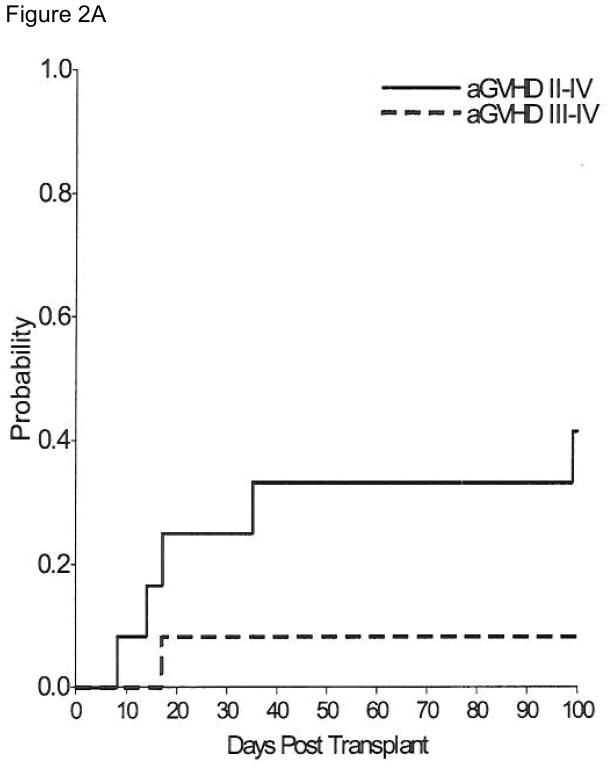
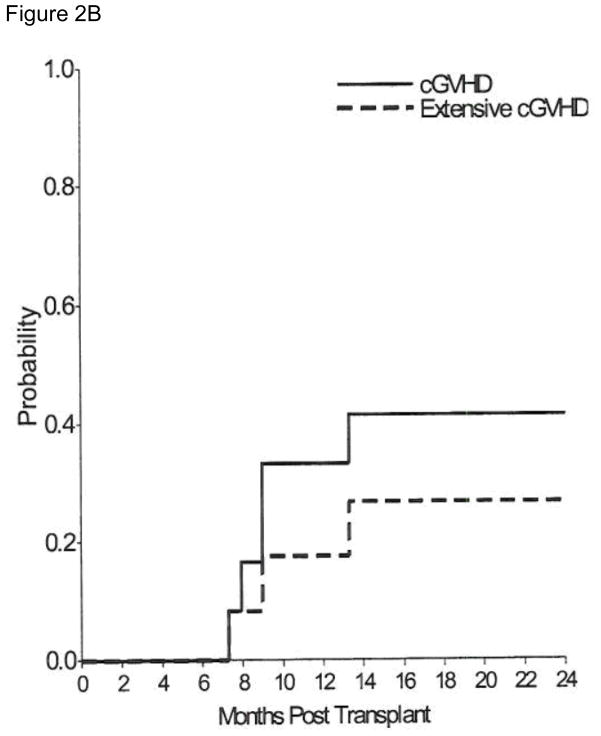
The curative potential of hematopoietic stem cell transplantation in patients with chronic granulomatous disease depends on availability of a suitable donor, successful donor engraftment, and maintenance of long-term donor chimerism. Twelve consecutive children (median age, 59.5 months; range, 8-140 months) with severe chronic granulomatous disease (serious bacterial/fungal infections pretransplantation; median, 3; range, 2-9) received myeloablative hematopoietic stem cell transplantation using sibling bone marrow ([SibBM]; n = 5), unrelated cord blood (UCB; n = 6), and sibling cord blood (n = 1) at our center between 1997 and 2010. SibBM and sibling cord blood were HLA matched at 6/6, whereas UCB were 5/6 (n = 5) or 6/6 (n = 1). Recipients of SibBM were conditioned with busulfan and cyclophosphamide ± anti-thymocyte globulin (ATG), whereas 6 of 7 cord blood recipients received fludarabine/busulfan/cyclophosphamide/ATG. Seven patients received granulocyte-colony stimulating factor-mobilized granulocyte transfusions from directed donors. The first 2 UCB recipients had primary graft failure but successfully underwent retransplantation with UCB. Highest acute graft-versus-host disease was grade III (n = 1). Extensive chronic graft-vs-host disease developed in 3 patients. All patients are alive with median follow-up of 70.5 months (range, 12-167 months) with high donor chimerism (>98%, n = 10; 94%, n = 1; and 92%, n = 1). Myeloablative hematopoietic stem cell transplantation led to correction of neutrophil dysfunction, durable donor chimerism, excellent survival, good quality of life, and low incidence of graft-vs-host disease regardless of graft source.
Published by Elsevier Inc.
Figures
References
-
- Rosenzweig SD. Inflammatory manifestations in chronic granulomatous disease (CGD) J Clin Immunol. 2008;28 (Suppl 1):S67–72. - PubMed
-
- Winkelstein JA, Marino MC, Johnston RB, Jr, et al. Chronic granulomatous disease. Report on a national registry of 368 patients. Medicine (Baltimore) 2000;79:155–169. - PubMed
-
- Kobayashi S, Murayama S, Takanashi S, et al. Clinical features and prognoses of 23 patients with chronic granulomatous disease followed for 21 years by a single hospital in Japan. EurJPediatr. 2008;167:1389–1394. - PubMed
-
- Liese J, Kloos S, Jendrossek V, et al. Long-term follow-up and outcome of 39 patients with chronic granulomatous disease. Journal of Pediatrics. 2000;137:687–693. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
