

Perspectives on the causes of childhood leukemia
- PMID: 22326931
- PMCID: PMC3839796
- DOI: 10.1016/j.cbi.2012.01.007
Perspectives on the causes of childhood leukemia
Abstract
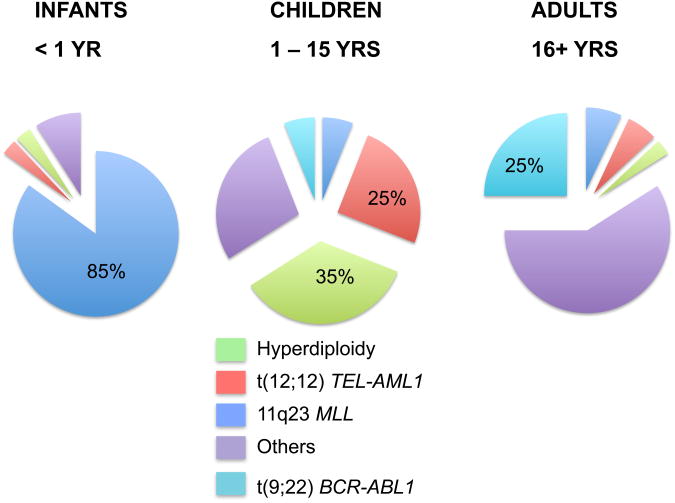
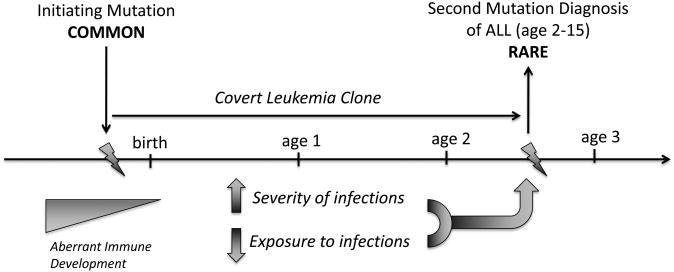
Acute leukemia is the most common cancer in children but the causes of the disease in the majority of cases are not known. About 80% are precursor-B cell in origin (CD19+, CD10+), and this immunophenotype has increased in incidence over the past several decades in the Western world. Part of this increase may be due to the introduction of new chemical exposures into the child's environment including parental smoking, pesticides, traffic fumes, paint and household chemicals. However, much of the increase in leukemia rates is likely linked to altered patterns of infection during early childhood development, mirroring causal pathways responsible for a similarly increased incidence of other childhood-diagnosed immune-related illnesses including allergy, asthma, and type 1 diabetes. Factors linked to childhood leukemia that are likely surrogates for immune stimulation include exposure to childcare settings, parity status and birth order, vaccination history, and population mixing. In case-control studies, acute lymphoblastic leukemia (ALL) is consistently inversely associated with greater exposure to infections, via daycare and later birth order. New evidence suggests also that children who contract leukemia may harbor a congenital defect in immune responder status, as indicated by lower levels of the immunosuppressive cytokine IL-10 at birth in children who grow up to contract leukemia, as well as higher need for clinical care for infections within the first year of life despite having lower levels of exposure to infections. One manifestation of this phenomenon may be leukemia clusters which tend to appear as a leukemia "outbreak" among populations with low herd immunity to a new infection. Critical answers to the etiology of childhood leukemia will require incorporating new tools into traditional epidemiologic approaches - including the classification of leukemia at a molecular scale, better exposure assessments at all points in a child's life, a comprehensive understanding of genetic risk factors, and an appraisal of the interplay between infectious exposures and the status of immune response in individuals.
Copyright © 2012 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
Figures
References
-
- Ries LAG, Smith MA, J G, Linet M, Tamra T, Young JL, Bunin GRe. In: Cancer Incidence and Survival among Children and Adolescents: United States SEER Progran 1975-1995. National Cancer Institute, editor. Bethesda, MD: 1999.
-
- Oeffinger KC, Mertens AC, Sklar CA, Kawashima T, Hudson MM, Meadows AT, Friedman DL, Marina N, Hobbie W, Kadan-Lottick NS, Schwartz CL, Leisenring W, Robison LL. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. 2006;355(15):1572–1582. - PubMed
-
- Linabery AM, Ross JA. Trends in childhood cancer incidence in the U.S. (1992-2004) Cancer. 2008;112(2):416–432. - PubMed
-
- Kaatsch P, Mergenthaler A. Incidence, time trends and regional variation of childhood leukaemia in Germany and Europe. Radiat Prot Dosimetry. 2008;132(2):107–113. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
