

Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor? Results of a longitudinal MRI and MRSI study
- PMID: 22331003
- PMCID: PMC3285390
- DOI: 10.1016/j.ijrobp.2011.11.030
Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor? Results of a longitudinal MRI and MRSI study
Abstract
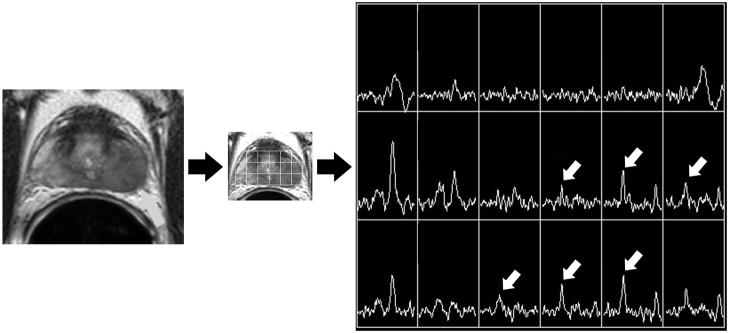
Purpose: To determine if local recurrence of prostate cancer after radiation therapy occurs at the same site as the primary tumor before treatment, using longitudinal magnetic resonance (MR) imaging and MR spectroscopic imaging to assess dominant tumor location.
Methods and materials: This retrospective study was HIPAA compliant and approved by our Committee on Human Research. We identified all patients in our institutional prostate cancer database (1996 onward) who underwent endorectal MR imaging and MR spectroscopic imaging before radiotherapy for biopsy-proven prostate cancer and again at least 2 years after radiotherapy (n = 124). Two radiologists recorded the presence, location, and size of unequivocal dominant tumor on pre- and postradiotherapy scans. Recurrent tumor was considered to be at the same location as the baseline tumor if at least 50% of the tumor location overlapped. Clinical and biopsy data were collected from all patients.
Results: Nine patients had unequivocal dominant tumor on both pre- and postradiotherapy imaging, with mean pre- and postradiotherapy dominant tumor diameters of 1.8 cm (range, 1-2.2) and 1.9 cm (range, 1.4-2.6), respectively. The median follow-up interval was 7.3 years (range, 2.7-10.8). Dominant recurrent tumor was at the same location as dominant baseline tumor in 8 of 9 patients (89%).
Conclusions: Local recurrence of prostate cancer after radiation usually occurs at the same site as the dominant primary tumor at baseline, suggesting supplementary focal therapy aimed at enhancing local tumor control would be a rational addition to management.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
There is no conflict of interest to disclose.
Figures
References
-
- American Cancer Society. Cancer Facts & Figures 2010. Atlanta: American Cancer Society; 2010. p. 23.
-
- Pouliot J, Kim Y, Lessard E, et al. Inverse planning for HDR prostate brachytherapy used to boost dominant intraprostatic lesions defined by magnetic resonance spectroscopy imaging. Int J Radiat Oncol Biol Phys. 2004;59:1196–1207. - PubMed
-
- van Lin EN, Futterer JJ, Heijmink SW, et al. IMRT boost dose planning on dominant intraprostatic lesions: Gold marker–based three-dimensional fusion of CT with dynamic contrast-enhanced and 1H-spectroscopic MRI. Int J Radiat Oncol Biol Phys. 2006;65:291–303. - PubMed
-
- Zelefsky MJ, Cohen G, Zakian KL, et al. Intraoperative conformal optimization for transperineal prostate implantation using magnetic resonance spectroscopic imaging. Cancer J. 2000;6:249–255. - PubMed
-
- Xia P, Pickett B, Vigneault E, et al. Forward or inversely planned segmental multileaf collimator IMRT and sequential tomotherapy to treat multiple dominant intraprostatic lesions of prostate cancer to 90 Gy. Int J Radiat Oncol Biol Phys. 2001;51:244–254. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
