

Drugs for relief of pain in patients with sciatica: systematic review and meta-analysis
- PMID: 22331277
- PMCID: PMC3278391
- DOI: 10.1136/bmj.e497
Drugs for relief of pain in patients with sciatica: systematic review and meta-analysis
Abstract
Objective: To investigate the efficacy and tolerability of analgesic and adjuvant pain drugs typically administered in primary care for the management of patients with sciatica.
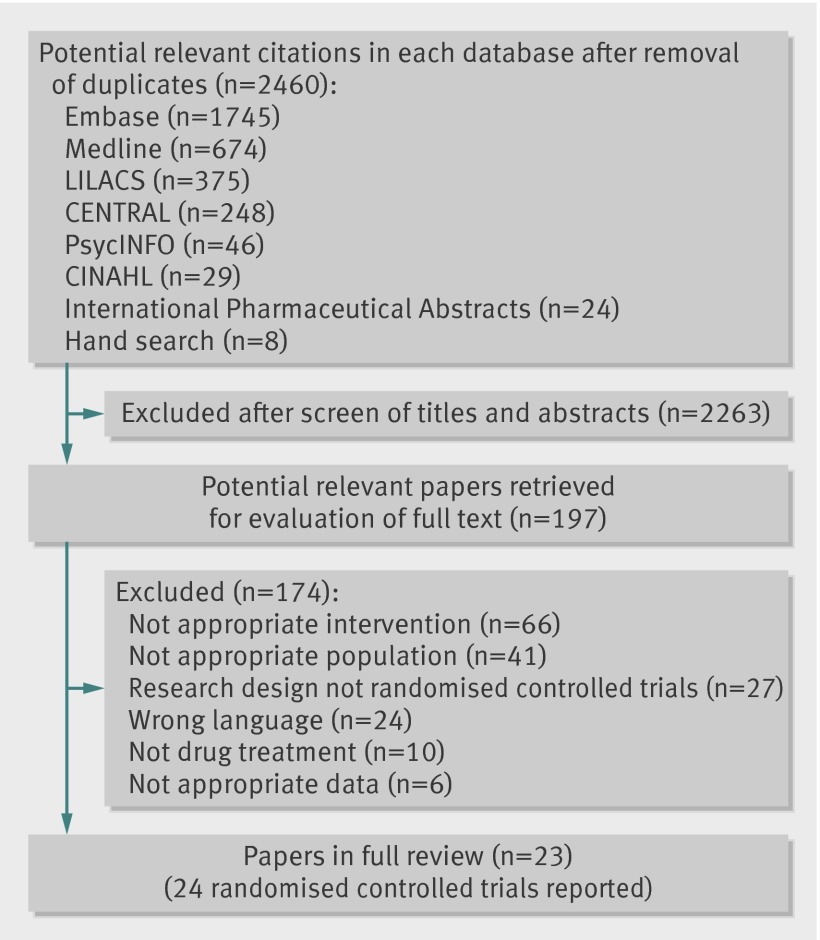
Design: Systematic review. Data source International Pharmaceutical Abstracts, PsycINFO, Medline, Embase, Cochrane Central Register of Clinical Trials (CENTRAL), CINAHL, and LILACS.
Study selection: Randomised controlled trials assessing the efficacy and tolerability of drugs versus placebo or other treatment for sciatica.
Data extraction: Two independent reviewers extracted data and assessed methodological quality using the PEDro scale. Pain and disability outcomes were converted to a common 0 to 100 scale. Data were pooled with a random effects model, and the GRADE approach was used in summary conclusions.
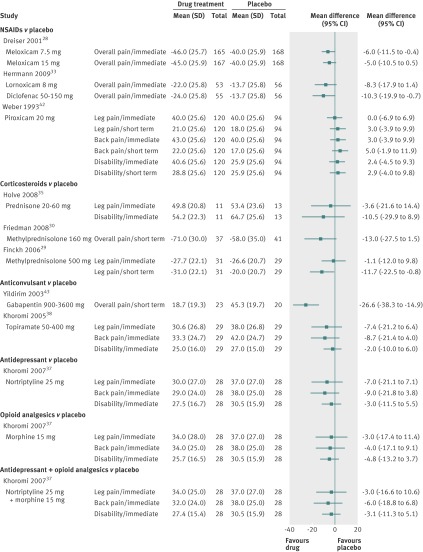
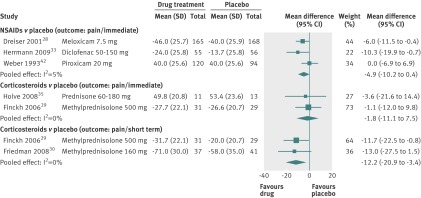
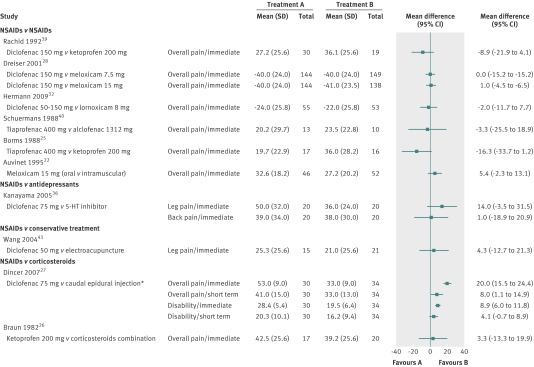
Results: Twenty three published reports met the inclusion criteria. The evidence to judge the efficacy of non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids, antidepressants, anticonvulsants, muscle relaxants, and opioid analgesics ranged from moderate to low quality. Most of the pooled estimates did not favour the active treatment over placebo. The pooled results of two trials of corticosteroids (mean difference in overall and leg pain -12.2, 95% confidence interval -20.9 to -3.4) and a single trial of the anticonvulsant gabapentin for chronic sciatica (mean difference in overall pain relief -26.6, -38.3 to -14.9) showed some benefits but only in the short term. The median rate of adverse events was 17% (interquartile range 10-30%) for the active drugs and 11% (3-23%) for placebo. Trial limitations included failure to use validated outcome measures, lack of long term follow-up, and small sample size.
Conclusions: As the existing evidence from clinical trials is of low quality, the efficacy and tolerability of drugs commonly prescribed for the management of sciatica in primary care is unclear.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Treating sciatica in the face of poor evidence.BMJ. 2012 Feb 13;344:e487. doi: 10.1136/bmj.e487. BMJ. 2012. PMID: 22331276 No abstract available.
References
-
- Konstantinou K, Dunn KM. Sciatica: review of epidemiological studies and prevalence estimates. Spine 2008;33:2464-72. - PubMed
-
- Balague F, Nordin M, Sheikhzadeh A, Echegoyen AC, Brisby H, Hoogewoud HM, et al. Recovery of severe sciatica. Spine 1999;24:2516-24. - PubMed
-
- Selim AJ, Ren XS, Fincke G, Deyo RA, Rogers W, Miller D, et al. The importance of radiating leg pain in assessing health outcomes among patients with low back pain. Results from the Veterans’ Health Study. Spine 1998;23:470-4. - PubMed
-
- Tubach F, Beaute J, Leclerc A. Natural history and prognostic indicators of sciatica. J Clin Epidemiol 2004;57:174-9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous