

Nonconvulsive status epilepticus: the encephalopathic pediatric patient
- PMID: 22331332
- PMCID: PMC9923578
- DOI: 10.1542/peds.2011-2067
Nonconvulsive status epilepticus: the encephalopathic pediatric patient
Abstract
Objective: A high prevalence of nonconvulsive status epilepticus (NCSE) has been reported in critically ill adults and neonates. Recent prospective pediatric studies focus on critically ill children and show wide variability in the frequency of NCSE. This study examines prevalence of pediatric NCSE regardless of inpatient setting and retrospectively identifies risk factors indicating a need for urgent continuous EEG.
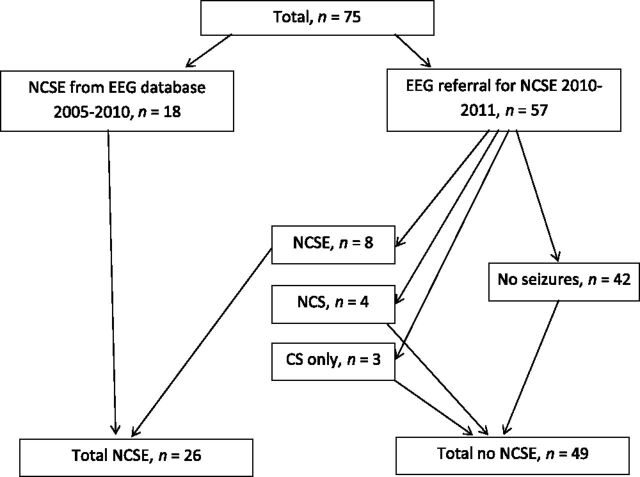
Methods: Medical records from patients aged 3 months to 21 years were identified either by (1) searching a clinical EEG database (n = 18) or (2) consecutive inpatient EEG referrals for NCSE over an 8-month period (n = 57).
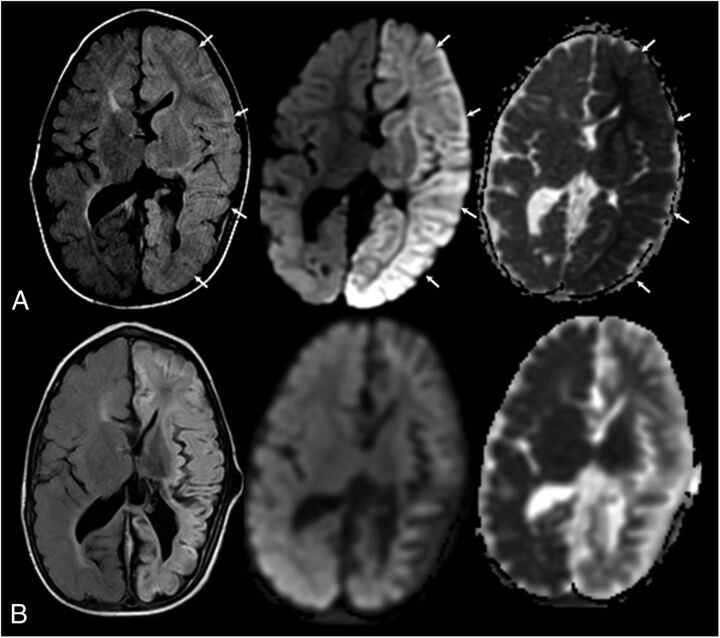
Results: Seventy-five children, mean age of 7.8 years, were studied. NCSE was identified in 26 patients (35%) and in 8 of 57 (14%) patients referred for possible NCSE. More than half of the patients referred were outside of the ICU. A witnessed clinical seizure was observed in 24 of 26 (92%) patients with NCSE. Acute cortical neuroimaging abnormalities were significantly more frequent in patients with NCSE. The presence of clinical seizures and acute neuroimaging abnormality was associated with an 82% probability of NCSE. All but 1 patient with NCSE had electrographic or electroclinical seizures within the first hour of monitoring.
Conclusions: A high prevalence of NCSE was observed, comparable to adult studies, but within a wider range of inpatient settings. Children with acute encephalopathy should undergo continuous EEG. This evaluation is more urgent if certain clinical risk factors are present. Optimal duration of monitoring and the effect of NCSE on prognosis should be studied.
Conflict of interest statement
Figures

References
-
- Shorvon S , Baulac M , Cross H , Trinka E , Walker M TaskForce on Status Epilepticus of the ILAE Commission for European Affairs . The drug treatment of status epilepticus in Europe: consensus document from a workshop at the first London Colloquium on Status Epilepticus. Epilepsia. 2008;49(7):1277–1285 - PubMed
-
- Walker M , Cross H , Smith S , et al. Nonconvulsive status epilepticus: Epilepsy Research Foundation workshop reports. Epileptic Disord. 2005;7(3):253–296 - PubMed
-
- Claassen J , Hirsch LJ , Frontera JA , et al. Prognostic significance of continuous EEG monitoring in patients with poor-grade subarachnoid hemorrhage. Neurocrit Care. 2006;4(2):103–112 - PubMed
-
- Shneker BF , Fountain NB . Assessment of acute morbidity and mortality in nonconvulsive status epilepticus. Neurology. 2003;61(8):1066–1073 - PubMed
-
- Pisani F , Sisti L , Seri S . A scoring system for early prognostic assessment after neonatal seizures. Pediatrics. 2009;124(4). Available at: www.pediatrics.org/cgi/content/full/124/4/e580 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
